
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2026 | 67 (1) | 40-46
Case report
Six-year follow-up of regenerative endodontics in a maxillary central incisor with apical periodontitis: Case report
Acompanhamento de seis anos de endodontia regenerativa em incisivo central superior com periodontite apical – Relato de Caso
a Federal University of Amazonas, School of Dentistry, Manaus, Brazil
b Ceproeducar, Manaus, Brazil
Ary Alves Mesquita-Júnior - aamesquitajunior@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 67
Issue - 1
Case report
Pages - 40-46
Go to Volume
Article History
Received on 21/06/2025
Accepted on 11/03/2026
Available Online on 23/04/2026
Keywords
Clinical Case Report
Six-year follow-up of regenerative endodontics in a maxillary central incisor with apical periodontitis: Case report
Acompanhamento de seis anos de endodontia regenerativa em incisivo central superior com periodontite apical – Relato de Caso
Ary Alves Mesquita-Júnior1,* 0009-0001-8444-4850
Ingrid Luiza Mendonça Cunha1 0000-0002-9222-6095
Norbi Rodrigues Correia2 0009-0007-4355-6657
Aida Renée Assayag Hanan1 0000-0001-6430-1791
Emílio Carlos Sponchiado Júnior1 0000-0001-7677-7682
1 Federal University of Amazonas, School of Dentistry, Manaus, Brazil.
2 Ceproeducar, Manaus, Brazil
Article history:
Received 21 June 2025
Accepted 11 March 2026
Available online 23 April 2026
Abstract
Regenerative endodontics is a biological alternative to apexification for managing immature teeth with pulp necrosis or irreversible pulpitis. This case report provides clinical relevance by demonstrating the 6-year success of a regenerative endodontic procedure using accessible materials and a reproducible protocol. A 12-year-old male presented with a traumatized maxillary central incisor showing crown discoloration, incomplete root formation, and a periapical lesion. Treatment was completed in two sessions. The first involved coronal access, irrigation with 2.5% sodium hypochlorite, and placement of a bi-antibiotic paste. In the second session, the paste was removed, and sodium hypochlorite was neutralized with saline solution. After drying, bleeding was induced, and a calcium silicate-based cement plug was placed, followed by coronal restoration. At the 6-year follow-up, the patient remained symptom-free, and imaging showed resolution of apical periodontitis, root elongation, and dentinal wall thickening. This case highlights the long-term success of regenerative procedures promoting root development and periapical healing.
Keywords: Apexification, Case reports, Dental pulp necrosis, Periapical periodontitis, Regenerative endodontics.
Resumo
A endodontia regenerativa constitui uma alternativa biológica à apexificação na abordagem de dentes imaturos com necrose pulpar ou pulpite irreversível. Este relato de caso apresenta relevância clínica ao demonstrar o sucesso, ao fim de seis anos, de um procedimento endodôntico regenerativo utilizando materiais acessíveis e um protocolo reprodutível. Um paciente do sexo masculino, de 12 anos, apresentou-se com um incisivo central maxilar traumatizado, com descoloração da coroa, formação radicular incompleta e uma lesão periapical. O tratamento foi realizado em duas sessões. Na primeira sessão, procedeu-se ao acesso coronário, irrigação com hipoclorito de sódio a 2,5% e aplicação de uma pasta biantibiótica. Na segunda sessão, a pasta foi removida e o hipoclorito de sódio neutralizado com solução salina. Após a secagem do canal, induziu-se hemorragia e colocou-se um tampão de cimento à base de silicato de cálcio, seguido da restauração coronária. Ao fim de seis anos, o paciente permanecia assintomático e os exames imagiológicos evidenciaram resolução da periodontite apical, alongamento radicular e espessamento das paredes dentinárias. Este caso evidencia o sucesso a longo prazo dos procedimentos regenerativos, promovendo o desenvolvimento radicular e a cicatrização periapical.
Palavras-chave: Apexificação,Relato de caso, Necrose pulpar dentária,Periodontite apical, Endodontia regenerativa.
Introduction
Endodontic treatment of teeth with incomplete root development and apical periodontitis is challenging because, in most cases, these teeth present thin dentinal walls, which preclude any type of canal enlargement and conventional obturation of the root canal system.1
Traditionally, teeth with incomplete root development were treated through apexification with repeated replacement of calcium hydroxide–based intracanal medicaments or by placement of a mineral trioxide aggregate (MTA) apical plug followed by root canal obturation. However, in these approaches, dentinal walls remained thin and fragile. With the advent of cell-based tissue engineering in endodontics, it became possible to change this scenario.1
Regenerative endodontic treatment has emerged as a promising alternative for the endodontic treatment of teeth with pulp necrosis and incomplete root development, as it may enable thickening of the internal dentinal walls in some cases.2 The concept underlying this approach is that the periapical environment can provide mesenchymal stem cells, biological mediators, and favorable conditions for the formation of new tissues within the root canal space. Studies have demonstrated that cells derived from the apical papilla, periodontal ligament, and even bone marrow are capable of migrating, proliferating, and contributing to angiogenic processes and cellular differentiation associated with tissue repair and dentinal development.3 - 5
For the success of this technique, several steps are considered fundamental: adequate disinfection of the root canal system, application of a scaffold to organize host stem cells, and effective coronal sealing.6 - 8 The literature also emphasizes the importance of long-term follow-up, since root maturation, formation of mineralized tissues, and resolution of periapical changes may occur gradually over several years.1, 9
Despite promising results, regenerative endodontic treatment may yield different outcomes, including resolution of periapical radiolucency without complete root development.10 Treatment failure is also possible, characterized by persistence of symptoms and periapical radiolucency, requiring further intervention.11
Although this therapeutic approach has been extensively investigated in recent years, there is still considerable variability in treatment protocols, material selection, and clinical indications.12 This study aims to report a clinical
case, written according to the CARE guidelines,13 of a patient presenting with symptomatic apical periodontitis and incomplete root development in the maxillary right central incisor, treated with regenerative endodontic treatment and followed for 6 years.
Case report
A 12-year-old male patient, systemically healthy, attended the endodontic clinic accompanied by his mother for emergency care. He reported pain in the labial mucosa adjacent to the maxillary right central incisor, with a history of trauma one year earlier. Clinical examination revealed a fractured, darkened crown associated with edema of the labial mucosa (Figure 1). Cold sensitivity testing was performed using a refrigerante spray (Endo Frost Roeko, Wilcos, Rio de Janeiro, Brazil), and the response was negative.

Figure 1. Initial clinical photograph showing crown discoloration and fracture on June 3, 2018.
Periapical radiographic examination revealed an extensive radiolucent area associated with the tooth, incomplete root development, and thin radicular walls (Figure 2). The periapical lesion was classified as score 5 according to the Periapical Index (PAI) proposed by Ørstavik et al.14 The patient had no systemic or hereditary diseases and no history of drug hypersensitivity.

Figure 2. Diagnostic periapical radiograph showing incomplete root development and apical periodontitis on June 3, 2018.
Regenerative endodontic treatment was proposed.
The patient and his legal guardian received detailed information about the proposed treatment and signed an informed consent form in accordance with the Brazilian National Health Council’s guidelines.
Initially, local anesthesia was achieved using one cartridge of lidocaine hydrochloride with epinephrine 36 mg (Alphacaine, DFL, Rio de Janeiro, Brazil), administered in the mucobuccal fold adjacent to the tooth and in the palatal gingival papilla. Access cavity preparation was performed with a spherical bur #1014 (KG Sorensen, Espírito Santo, Brazil), and cavity refinement was carried out with a non-cutting tapered bur #3083 (KG Sorensen, Espírito Santo, Brazil), under high-speed rotation with water cooling. Absolute isolation was achieved using a rubber dam sheet (Madeitex, São Paulo, Brazil) and clamp #211 (Golgran, São Paulo, Brazil).
Chemical preparation was performed using 2.5% sodium hypochlorite solution (Asfer, São Paulo, Brazil), and no mechanical instrumentation of the root canal was carried out.
Prior to filling the canal with intracanal medication, drying was performed using sterile paper points size #80 (Dentsply Sirona, Switzerland). Subsequently, a bi-antibiotic paste (ciprofloxacin and metronidazole) was inserted into the canal using a Lentulo spiral size #40 (Dentsply Sirona, Switzerland).
For temporary coronal sealing between appointments, sterile cotton pellets and a restorative glass ionomer cement (Maxxion R, FGM, Santa Catarina, Brazil) were used. At the second appointment, 28 days after the first, the patient reported no pain, and clinical examination revealed no intraoral edema. Local anesthesia was performed using mepivacaine without vasoconstrictor (Mepivacaine 3% – Nova DFL, Rio de Janeiro, Brazil). Absolute isolation and reopening of the access cavity were performed using the same protocol as during the first appointment.
Irrigation was carried out with 2.5% sodium hypochlorite solution (Soda Clorada, Asfer, São Paulo, Brazil), followed by 17% EDTA solution (Asfer, São Paulo, Brazil), and a final irrigation with sterile saline solution (Eurofarma, Amazonas, Brazil).
Subsequently, the root canal system was dried using sterile paper points size #80 (Dentsply Sirona, Switzerland).
A long gingival needle (38 mm × 0.4 mm, 27G; Dencojet, Nova DFL, Rio de Janeiro, Brazil) was introduced 2 mm beyond the working length to induce bleeding and fill the entire canal space. At the level of the cemento-enamel junction, a plug of MTA (Angelus, Paraná, Brazil) was placed to seal the canal entrance (Figure 3), followed by placement of a restorative glass ionomer cement (Maxxion R, FGM, Santa Catarina, Brazil).
After acid etching with 37% phosphoric acid (Condac 37%, FGM, Santa Catarina, Brazil) for 15 seconds on dentin and 30 seconds on enamel, an adhesive system (Single Bond Universal, 3M do Brasil, Sumaré, São Paulo, Brazil) was applied. The coronal restoration was completed using the incremental technique with composite resin A3 (Z350, 3M do Brasil, Sumaré, São Paulo, Brazil). Light curing was performed using a Radii Cal curing unit (SDI, Santa Catarina, Brazil) (Figure 4). The patient was dismissed, and the legal guardian was informed that periodic clinical and radiographic follow-up appointments would be required. At the 13-month follow-up, the patient was asymptomatic, with radiographic evidence of bone formation in the periapical region (Figure 5). At subsequente follow-ups at 5 years (Figure 6) and 6 years (Figures 7 and 8), the patient remained asymptomatic and radiographically free of signs of apical periodontitis. Additionally, imaging revealed the formation of a mineralized barrier between the apical plug and the remaining portion of the root, a slight increase in dentinal wall thickness, and mild elongation of the treated tooth root.

Figure 3. Cervical plug placed with calcium silicate based cement on June 30, 2018.
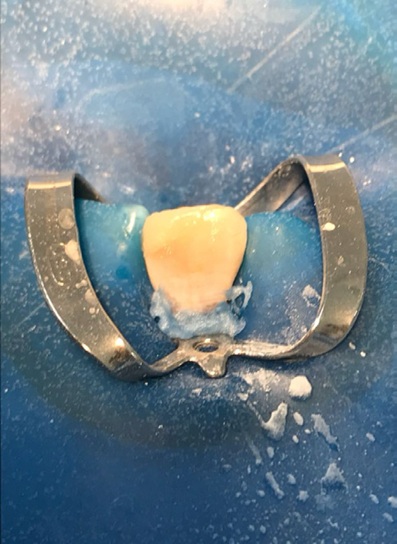
Figure 4. Coronal sealing was performed with resinmodified glass ionomer cement on June 30, 2018.

Figure 5. Thirteen-month follow-up radiograph obtained on July 27, 2019.

Figure 6. Five-year follow-up radiograph obtained on July 20, 2023.

Figure 7. Six-year follow-up radiograph obtained on July 30, 2024.

Figure 8. Clinical photograph showing the restored tooth and ongoing orthodontic treatment at the six-year follow-up (July 30, 2024).
Discussion and conclusions
Endodontic treatment of teeth with incomplete root development and apical periodontitis remains challenging because, despite the availability of traditional treatment techniques such as apexification, none of these allows further root development or an increase in radicular dentinal wall thickness.1, 15
This therapeutic modality was selected in the present case due to root immaturity, wide apical foramen, and extensive periapical radiolucency, with the aim of promoting root development and preserving the affected tooth. However, after six years of follow-up, complete apical closure was not observed.
Instead, the formation of a mineralized barrier between the coronal plug and the root apex was identified, along with a slight increase in root length, complete periapical healing, and absence of clinical symptoms. According to classical studies,10, 16 these findings constitute a well-established measure of clinical success, even in the absence of full root maturation.
According to the classification proposed by Chen et al.10, the outcomes of regenerative endodontic treatment can be grouped into five patterns: type 1, increased canal wall thickness with continued root development; type 2, a blunted and closed apex without significant root development; type 3, continued root development with a persistent open apical foramen; type 4, severe intracanal calcification; and type 5, a hard tissue barrier formed between the MTA plug and the root apex.
In the present case, radiographic evaluation from the 13-month follow-up onward demonstrated a radiopaque image suggestive of mineralized barrier formation in this region, consistente with the type-5 pattern.
A similar outcome was reported by Nosrat et al.17, reinforcing the variability of clinical responses to regenerative therapies and prompting a re-evaluation of the indications for traditional techniques, such as apexification or conventional root canal obturation. Nevertheless, despite this unpredictability, such variations might be attributed to differences in treatment protocols, stages of root development, pulpal conditions, and the extent of periapical pathology.12 In the study by Nosrat et al., the need for reintervention after six years was attributed to loss of coronal sealing associated with caries development and the consequent risk of recontamination of the root canal system.
Although the initial objective of this case, thickening of dentinal walls and apical closure, was not fully achieved, Kahler et al.18 emphasize that additional interventions are not required when there is clear evidence of resolution of periapical pathology, even in the absence of significant root maturation.
This understanding supports the clinical management adopted in the present report.
The protocol described in this case followed the recommendations of the American Association of Endodontists (AAE) that were in effect at the time of treatment.19, 20 Adequate disinfection of the root canal system is essential; however, conventional chemomechanical preparation may further weaken thin dentinal walls. Therefore, according to Wei et al.21, minimal instrumentation may be indicated. Sodium hypochlorite at low concentrations does not exert deleterious effects on stem cells derived from the apical papilla, and its neutralization before bleeding induction by a final rinse with sterile saline solution is recommended.22, 23
The use of 17% EDTA in regenerative endodontic procedures plays an essential role by neutralizing sodium hypochlorite and inducing the release of growth factors from dentin, particularly transforming growth factor beta (TGF-β).24 To further enhance canal disinfection, a bi-antibiotic paste was used in this case, as it effectively inhibits bacterial growth within the root canal system.24
Once a suitable environment for cellular activity has been established, a scaffold must be introduced to enable interaction between stem cells and growth factors. In the presente case, a blood clot was used as the scaffold, as it has demonstrated satisfactory clinical outcomes, does not require additional equipment or resources, is easy to obtain, and presents similar clinical and radiographic results when compared with other scaffolds, such as platelet-rich fibrin and platelet-rich plasma.6, 25, 26 MTA was used as a coronal barrier to protect the scaffold due to its biologically active properties, lack of cytotoxicity, and adequate marginal sealing ability.16, 27
The literature indicates that regenerative endodontic treatment results in high rates of periapical lesion resolution, with several clinical series reporting healing of periapical pathology even in the absence of complete root maturation.10, 17, 18 However, outcomes related to root development are heterogeneous, and only a limited number of cases demonstrate significant dentinal wall thickening or measurable root elongation.29 Failure rates are reported and are mainly associated with persistente infection, difficulty in inducing bleeding, loss of coronal sealing, or development of canal obliteration due to calcification.10, 17, 30 Even in cases of treatment failure, reintervention using traditional techniques, such as MTA apexification or conventional root canal obturation, remains a predictable and viable alternative for tooth preservation.17, 18
Regenerative endodontic treatment represents a promising alternative for treating teeth with incomplete root development, despite the different possible clinical outcomes associated with this therapeutic approach. Long-term follow-up is essential to properly assess periapical healing, root maturation, and the survival rate of teeth treated with regenerative endodontic procedures, as treatment failure may occur due to factors such as persistent infection, external or internal resorption, and caries development.28 In cases of treatment failure, characterized by the persistence of clinical symptoms and periapical pathology, reintervention remains feasible using alternative treatment techniques. In the case presented, after 6 years of follow-up, the patient remained asymptomatic, with a radiopaque image suggestive of mineralized barrier formation, slight increase of dentinal wall thickness, and mild root elongation, and no radiographic signs of periapical disease.
References
1. Saad W, Almaslamani M, Saleh AR. Revascularization of a Permanent Tooth with Necrotic Pulp and Apical Periodontitis. Clin Cosmet Investig Dent. 2024;16:227-35.
2. Murray PE. Platelet-Rich Plasma and Platelet-Rich Fibrin Can Induce Apical Closure More Frequently Than Blood-Clot Revascularization for the Regeneration of Immature Permanent Teeth: A Meta-Analysis of Clinical Efficacy. Front Bioeng Biotechnol. 2018;6:139.
3. Orduña JFG, García MG, Dominguez P, Bucheli JC, Biedma BM, Sans FA, et al. Successful pulp revascularization of na autotransplantated mature premolar with fragile fracture apicoectomy and plasma rich in growth factors: a 3-year follow-up. Int Endod J. 2020;53:421-33.
4. Gaviño-Orduña JF, Fernández-Guallart I, Caviedes-Bucheli J, Espadas-Garcia M, López-López J. Regenerative endodontic procedure combined with apical surgery of a necrotic permanent incisor with extensive periapical lesion using plasma rich in growth factors (PRGF): A Case report with 6 years post-op evaluation using CBCT. J Clin Exp Dent. 2021;13:e620-5.
5. Ramezani M, Sanaei-Rad P, Hajihassani N. Revascularization and vital pulp therapy in immature molars with necrotic pulp and irreversible pulpitis: A case report with two-year follow-up. Clin Case Rep. 2020;8:206-10.
6. Lovelace TW, Henry MA, Hargreaves KM, Diogenes A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J Endod. 2011;37:133-8.
7. Kim SG. Infection and Pulp Regeneration. Dent J (Basel). 2016;4:4.
8. Torabinejad M, Nosrat A, Verma P, Udochukwu O. Regenerative Endodontic Treatment or Mineral Trioxide Aggregate Apical Plug in Teeth with Necrotic Pulps and Open Apices: A Systematic Review and Meta-analysis. J Endod. 2017;43:1806-20.
9. Sponchiado-Júnior EC, Vieira WA, Frozoni M, Herkrath FJ, de-Jesus-Soares A. CONSORT Compliance in Randomized Clinical Trials of Regenerative Endodontic Treatments of Necrotic Immature Teeth: A Scoping Review. J Endod. 2021;47:1751-66.
10. Chen MYH, Chen KL, Chen CA, Tayebaty F, Rosenberg PA, Lin LM. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int Endod J. 2012;45:294-305.
11. Alfahadi HR, Al-Nazhan S, Alkazman FH, Al-Maflehi N, Al-Nazhan N. Clinical and radiographic outcomes of regenerative endodontic treatment performed by endodontic postgraduate students: a retrospective study. Restor Dent Endod. 2022;47:e24.
12. Lin LM, Kahler B. A review of regenerative endodontics: current protocols and future directions. J Istanb Univ Fac Dent. 2017;51(3 Suppl 1):S41-51.
13. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, et al. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development. Glob Adv Health Med. 2013;2:38-43.
14. Ørstavik D, Kerekes K, Eriksen HM. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986;2:20-34.
15. Asgary S, Shamszadeh S, Nosrat A, Aminoshariae A, Sabeti M. Management Strategies for Immature Teeth with Pulp Necrosis: An Umbrella Review of Systematic Reviews. Iran Endod J. 2024;19:242-53.
16. Banchs F, Trope M. Revascularization of immature permanente teeth with apical periodontitis: new treatment protocol? J Endod. 2004;30:196-200.
17. Nosrat A, Homayounfar N, Oloomi K. Drawbacks and unfavorable outcomes of regenerative endodontic treatments of necrotic immature teeth: a literature review and report of a case. J Endod. 2012;38:1428-34.
18. Kahler B, Mistry S, Moule A, Ringsmuth AK, Case P, Thomson A, et al. Revascularization outcomes: a prospective analysis of 16 consecutive cases. J Endod. 2014;40:333-8.
19. Saoud TMA, Ricucci D, Lin LM, Gaengler P. Regeneration and Repair in Endodontics-A Special Issue of the Regenerative Endodontics-A New Era in Clinical Endodontics. Dent J (Basel). 2016;4:3.
20. Duggal M, Tong HJ, Al-Ansary M, Twati W, Day PF, Nazzal H. Interventions for the endodontic management of non-vital traumatised immature permanent anterior teeth in children and adolescents: a systematic review of the evidence and guidelines of the European Academy of Paediatric Dentistry. Eur Arch Paediatr Dent. 2017;18:139-51.
21. Wei X, Yang M, Yue L, Huang D, Zhou X, Wang X, et al. Expert consensus on regenerative endodontic procedures. Int J Oral Sci. 2022;14:55.
22. Dos Reis-Prado AH, Abreu LG, Fagundes RR, Oliveira SC, Bottino MC, Ribeiro-Sobrinho AP, et al. Influence of ethylenediaminetetraacetic acid on regenerative endodontics: A systematic review. Int Endod J. 2022;55:579- 612.
23. Parchami K, Dastorani M, Barati M. What is the impact of Endodontic Irrigant Solutions on the Viability of Stem Cells from Apical Papilla in an in-vitro setting: A Systematic Review. Saudi Dent J. 2024;36:1170-8.
24. Montero-Miralles P, Martin-Gonzalez J, Alonso-Ezpeleta O, Jimenez-Sanchez MC, Velasco-Ortega E, Segura-Egea JJ. Effectiveness and clinical implications of the use of topical antibiotics in regenerative endodontic procedures: a review. Int Endod J. 2018;51:981-8.
25. Rios-Osorio N, Caviedes-Bucheli J, Jimenez-Pena O, Orozco-Agudelo M, Mosquera-Guevara L, Jimenez-Castellanos FA, et al. Comparative outcomes of platelet concentrates and blood clot scaffolds for regenerative endodontic procedures: A systematic review of randomized controlled clinical trials. J Clin Exp Dent. 2023;15:e239-49.
26. Thakkar S, Naik S, Nadig B, Bellal S, Thaliyil A. A comparative clinico-radiographic analysis of regenerative endodontic procedure on immature necrotic permanent teeth using blood clot and PRF as scaffold: A retrospective study. Saudi Dent J. 2023;35:753-9.
27. Gunal E, Bezgin T, Ocak M, Bilecenoglu B. Effects of various thicknesses and levels of mineral trioxide aggregate coronal plugs on nanoleakage and fracture resistance in revascularization: An in vitro study. Aust Endod J. 2021;47:608-15.
28. Lee C, Song M. Failure of Regenerative Endodontic Procedures: Case Analysis and Subsequent Treatment Options. J Endod. 2022;48:1137-45.
29. Jeeruphan T, Jantarat J, Yanpiset K, Suwannapan L, Khewsawai P, Hargreaves KM. Mahidol study 1: comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: a retrospective study. J Endod. 2012;38:1330-6.
30. Almutairi W, Yassen GH, Aminoshariae A, Williams KA, Mickel A. Regenerative Endodontics: A Systematic Analysis of the Failed Cases. J Endod. 2019;45:567-77.
Ary Alves Mesquita-Júnior
E-mail address: aamesquitajunior@gmail.com
CRediT authorship contribution statement
Ary Alves Mesquita-Júnior: Conceptualization, Investigation, Methodology, Writing – original draft. Ingrid Luiza Mendonça Cunha: Conceptualization, Methodology, Writing – original draft. Norbi Rodrigues Correia: Conceptualization, Methodology, Writing – review & editing. Aida Renée Assayag Hanan: Conceptualization, Methodology, Writing – review & editing. Emílio Carlos Sponchiado Júnior: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
1646-2890/© 2026 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).