
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2026 | 67 (1) | 27-33
Case report
Oral verrucous carcinoma in unusual locations: Two case reports
Carcinoma verrucoso oral em localizações incomuns: Dois casos clínicos
a Oral and Maxillofacial Surgery Outpatient Clinic of the Lauro Wanderley University Hospital, Federal University of Paraíba (HULW/UFPB), João Pessoa, Paraíba, Brazil.
b Piracicaba Dental School, University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil.
Josivaldo Bezerra Soares - josivaldo.soares@academico.ufpb.br
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 67
Issue - 1
Case report
Pages - 27-33
Go to Volume
Article History
Received on 09/03/2025
Accepted on 25/02/2026
Available Online on 03/04/2026
Keywords
Clinical Case Report
Oral verrucous carcinoma in unusual locations: Two case reports
Carcinoma verrucoso oral em localizações incomuns: Dois casos clínicos
Josivaldo Bezerra Soares1,2,* 0000-0002-0283-5090
Beatriz Medeiros Batista1 0009-0000-6392-919X
Sérgio Cantídio Carneiro Morais1 0000-0002-4945-9555
Cícera Dalylla Lopes Ferreira1 0000-0001-8726-8277
Katia Caetana Pereira1 0000-0002-0781-9970
Paulo Rogério Ferreti Bonan2 0000-0002-4449-4343
1 Oral and Maxillofacial Surgery Outpatient Clinic of the Lauro Wanderley University Hospital, Federal University of Paraíba (HULW/UFPB),
João Pessoa, Paraíba, Brazil.
2 Piracicaba Dental School, University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil.
Article history:
Received 9 March 2025
Accepted 25 February 2026
Available online 2 April 2026
Abstract
Verrucous carcinoma is a rare, distinct, well-differentiated variant of squamous cell carcinoma, characterized by slow growth, local invasiveness, and low metastatic potential. The tumor predominantly affects the buccal mucosa, followed by the mandibular alveolar ridge, gingiva, and tongue. We report two cases of oral verrucous carcinoma in unusual locations. Case 1 presented as a white verrucous lesion on the lower lip, while Case 2 manifested as a palatal lesion with a cauliflower-like verrucous surface. Microscopically, both cases exhibited an exophytic tumor with a verruciform architecture and invasive growth through broad, bulbous rete ridges. Therefore, the definitive diagnosis for both patients was verrucous carcinoma. Distinguishing verrucous carcinoma from other verrucous lesions poses a significant challenge for pathologists. A deep biopsy incorporating adjacent normal tissue is mandatory for accurate differential diagnosis and to rule out hybrid carcinoma.
Keywords: Mouth,Oral and maxillofacial pathology,Squamous cell carcinoma of head,and neck,Verrucous carcinoma.
Resumo
O carcinoma verrucoso é uma variante rara, distinta e bem diferenciada do carcinoma de células escamosas, que apresenta crescimento lento, padrão de invasão local e baixo potencial metastático. O tumor tem predileção pela mucosa bucal, seguindo-se a crista alveolar mandibular, a gengiva e a língua. Apresentamos dois casos de carcinoma verrucoso oral em localizações incomuns. O caso 1 mostrou uma lesão verrucosa branca no lábio inferior, enquanto o caso 2 revelou uma lesão no palato com uma superfície verrucosa semelhante a couve-flor. Microscopicamente, ambos os casos demonstraram um tumor exofítico com uma superfície verruciforme e um crescimento invasivo com cristas epiteliais bulbosas e largas. Portanto, o diagnóstico definitivo em ambos os casos foi carcinoma verrucoso. O diagnóstico diferencial entre carcinoma verrucoso e outras lesões verrucosas permanece um desafio para os patologistas. Uma biópsia profunda com margens de tecido normal adjacente é essencial para o diagnóstico diferencial e exclusão de um carcinoma híbrido.
Palavras-chave: Boca, Patologia oral e maxilofacial, Carcinoma de células escamosas de cabeça e pescoço, Carcinoma verrucoso.
Introduction
Verrucous carcinoma (VC), initially described by Ackerman in 1948, is a rare, distinct, well-differentiated variant of squamous cell carcinoma (SCC), with specific morphological and clinical characteristics.1, 2 Unlike conventional SCC, VC exhibits slow growth, a local invasion pattern, and low potential for regional and distant metastases.3 Typically, VC affects middle-aged and elderly adults, with a peak in the sixth and seventh decades of life, and is more prevalent in men than in women.4, 5
Regarding location, VC predominantly affects the mucous membranes of the head and neck region, particularly the oral cavity, larynx, hypopharynx, and trachea.6, 7 In the oral cavity, the most common sites are the buccal mucosa, followed by the mandibular alveolar ridge, gingiva, and tongue.2, 8 Clinically, oral lesions present as asymptomatic, well-demarcated exophytic growths with superficial papillary or verruciform projections, often resembling cauliflower. The lesions are usually white but can appear pink or erythematous.9 VC accounts for approximately 2−12% of all oral carcinomas.10 Although the etiology is not well understood, risk factos commonly associated with VC development include smoking, tobacco chewing, alcohol consumption, and poor oral hygiene. Other etiological factors include human papillomavirus (HPV), areca nut chewing, immunosuppression, oral leukoplakia, and oral submucous fibrosis.11, 12 The treatment of choice for oral VC is surgical excision with wide margins.13
Overall, the prognosis is favorable, with a 5-year survival rate of approximately 80%; however, the recurrence rate varies from 30% to 50%.14, 15
This paper presents two cases of oral VC in elderly men occurring in unusual locations — the palate and the lower lip, followed by a literature review emphasizing clinical features, histological findings, and treatment modalities.
Case reports
Case 1
A 77-year-old male patient was referred to the (placeholder for the institution’s name) for evaluation of a white verrucous lesion on the lower lip with a duration of approximately 1 year.
The medical history revealed no systemic diseases or drug allergies. In addition, the patient reported a 63-year history of smoking. On physical examination, no regional lymphadenopathy was observed. A whitish exophytic lesion was present on the vermilion border and mucosa of the lower lip. The plaque was thick and well-circumscribed, with a papillary surface and a sessile base, measuring approximately 3 cm in diameter (Figure 1). Based on these findings, a clinical hypothesis of VC was established. An incisional biopsy was performed under local anesthesia, and the specimen was submitted for histopathological examination.

Figure 1. Extraoral examination showing a White verrucous lesion on the lower lip.
Microscopic examination demonstrated a well-differentiated stratified squamous epithelium with marked superficial keratinization and verrucous exophytic projections, consistente with the “church spire” sign. Additionally, the
hyperplastic epithelium exhibited endophytic growth with broad, bulbous epithelial ridges pushing into the underlying connective tissue (Figure 2). At higher magnification, mild cytologic atypia was observed in the basal layer, with no evidence of overt invasion (Figure 3). The underlying connective tissue showed a chronic inflammatory infiltrate composed predominantly of lymphocytes, as well as rich vascularity and no lymphovascular or perineural invasion. Therefore, a histopathologic diagnosis of VC was confirmed. The patient was referred to a head and neck surgeon and is currently undergoing treatment.
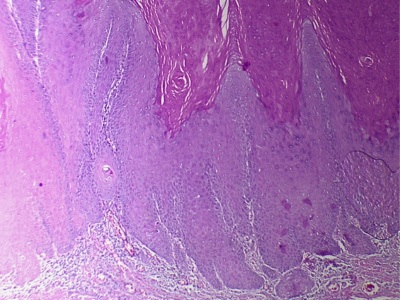
Figure 2. Photomicrograph showing exophytic tumor with church spire sign and broad, bulbous epitelial ridges that appeared to push against the underlying connective tissue (H&E, 40x).
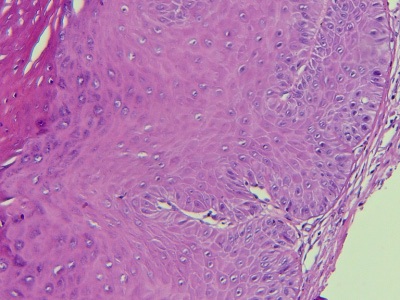
Figure 3. Photomicrograph showing mild cytologic atypia in the basal layer and absence of frank invasion (H&E, 100x).
Case 2
A 71-year-old male patient presented to the (placeholder for the institution’s name), complaining of a lesion on the palate with unknown duration. During the anamnesis, the medical history was non-contributory, although the patient reported a long-term habit of smoking and chewing tobacco. Extraoral examination revealed no edema or facial asymmetry; however, the right submandibular lymph nodes were enlarged. Intraoral examination revealed an extensive tumor mass located on the palate, extending to the upper alveolar ridge and buccal vestibule. The lesion presented exophytic growth, reddish- white coloration, and a cauliflower-like verrucous surface (Figure 4). Therefore, the diagnostic hypothesis was VC. An incisional biopsy was performed under local anesthesia, and the specimen was sent for histopathological analysis. Histological analysis revealed acanthotic stratified squamous epithelium with hyperparakeratosis and a verruciform surface, resembling the blunt variant of verrucous hyperplasia (Figure 5). The epithelium showed moderate dysplasia and invasive growth, with blunt, broad epithelial ridges exhibiting pushing borders into the underlying connective tissue, compared to the adjacent normal epithelium (Figure 6). The lamina propria was fibrous, containing dense bundles of collagen fibers and minimal vascularity. Based on the findings, a diagnosis of VC was established. The patient was referred for head and neck surgery and is currently undergoing treatment.

Figure 4. Intraoral examination showing a lesion on the palate extending to the upper alveolar ridge and buccal vestibule, displaying a cauliflower-like verrucous surface.
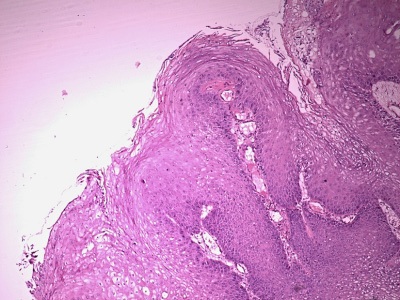
Figure 5. Photomicrograph revealing exophytic tumor with parakeratosis and verruciform surface, similar to the blunt variant of verrucous hyperplasia (H&E, 40x)
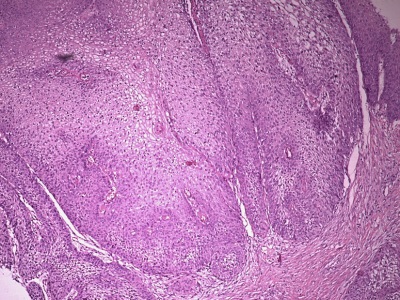
Figure 6. Photomicrograph showing moderate dysplasia and an invasive growth with blunt, broad epithelial ridges (H&E, 100x).
Discussion and conclusions
In 1948, Ackerman1 first described VC as an exophytic tumor with a verrucoid or cauliflower-like appearance, slow growth, local invasiveness, and low metastatic potential.15 The clinical characteristics of VC contrast with the ulcerative and nodular appearance of conventional SCC, which is the most frequente malignancy of the oral mucosa.15, 16 VC accounts for approximately 2−6% of all oral cavity carcinomas and is more prevalente in elderly men, usually in the 6th and 7th decades of life, as observed in the present cases.6, 7 The most common intraoral locations are the buccal mucosa, gingiva, and tongue; this distribution differs from our cases, which involved the palate and lower lip.17
The etiology of VC remains controversial, but it is associate with poor oral hygiene, alcohol consumption, smoking (bidis and cigarettes), and, predominantly, smokeless tobacco and areca nut chewing. These etiological factors have been implicated in the malignant transformation of leukoplakia, erythroleukoplakia, submucous fibrosis, lichen planus, and oral lichenoid reaction.16, 18 - 20 Conversely, approximately 20% of patients affected by VC do not report any predisposing factors. 6, 15 Regarding proliferative verrucous leukoplakia, the development of VC from this potentially malignant disorder is less common, particularly as proliferative verrucous leukoplakia is not typically associated with tobacco use.21
Another predisposing factor suggested in the etiopathogenesis of VC is the human papillomavirus (HPV), which has been detected in tumor cells.22, 23 Greere et al.24 demonstrated the presence of HPV in approximately 20% of VC cases, especially subtypes 16 and 18. Although HPV’s influence on the oncogenesis of VC is less significant compared to SCC, studies indicate that the pathogenesis of VC involves the abrogation of a tumor suppressor gene by oncogenic HPV subtypes.19, 25
Additionally, physical factors, such as irritation and repetitive mechanical trauma, may contribute to VC development, alongside chronic inflammatory processes like osteomyelitis, fistulas, ulcers, and lipoid necrobiosis.25, 27 In the cases presented herein, the only etiological factors identified were tobacco use and poor oral hygiene, corroborating literature that smoking and chewing tobacco represent the primary carcinogenic factos in VC.
Regarding differential diagnosis, VC mimics several benign oral tumors; thus, lesions with a similar appearance must be considered in the clinical and histopathological differential diagnosis, such as squamous papilloma, condyloma acuminatum, focal epithelial hyperplasia, pseudoepitheliomatous hyperplasia, chronic hyperplastic candidiasis, verrucous hyperplasia, and proliferative verrucous leukoplakia.28 - 30 Furthermore, a distinction should be made between VC and conventional SCC, especially with SCC that exhibits a “verrucoid” appearance.31 The accurate diagnosis of VC can be challenging and requires an adequate incisional biopsy, as well as close cooperation between the clinician and the pathologist. In this context, superficial biopsies may microscopically display only benign features, such as hyperkeratosis, acanthosis, and papillomatosis, leading to an erroneous diagnosis of benign squamous proliferation. Therefore, a broad and deep biopsy is required to obtain an accurate microscopic diagnosis, avoiding the need for multiple biopsies and the misinterpretation of a malignant process as benign.1, 29, 32, 33
The definitive diagnosis of VC is usually based on histopathological examination of clinically suspicious oral lesions and requires the identification of the histological criteria described by Ackerman.1 Histopathologically, VC typically presents with predominantly exophytic growth of well-differentiated hyperplastic epithelium, exhibiting a heavily keratinized or parakeratinized surface and sharp or blunt epithelial projections. In addition, scarce fibrovascular cores are noted, as well as numerous clefts between epithelial projections filled with keratin (keratin plugging). An intense subepithelial chronic inflammatory infiltrate is often present. Other important histopathological features include an intact basement membrane, preservation of stratification, minimal or absent atypia, and bulbous epithelial ridges, displaying an endophytic growth pattern that compresses the underlying connective tissue.13, 31, 34, 35
The abrupt transition between the adjacent normal epithelium and the endophytic growth of the lesion is considered a critical feature for distinguishing VC from benign verrucous processes.36 The cases presented herein showed microscopic findings consistent with these aforementioned features.
Several studies have demonstrated cases of SCC arising within VC. It is suggested that VC may arise de novo or from epitelial dysplasia and subsequently transform into conventional SCC, presenting more or less differentiated foci of SCC. In this context, the presence of at least one focus of SCC transformation within a VC lesion characterizes a hybrid carcinoma.30, 37, 38 In fact, VC cases often present microinvasion, indicating that atypical basal cells have acquired invasive properties.39 During histopathological examination, it is mandatory to rule out SCC and hybrid carcinoma, which require staging and treatment as conventional SCC due to the greater metastatic potential.31 To this end, large and deep biopsies are essential, as invasion may be missed in small and superficial specimens, making it unfeasible to exclude an underlying conventional carcinoma.31 Gokavarapu et al.40 reported that approximately 50% of cases clinically diagnosed as oral VC or its benign precursors actually represented hybrid carcinomas. Therefore, a thorough microscopic examination of the entire specimen, using serial sections to examine deeper tissues, is crucial for identifying potential invasive components.9, 40 If hybrid VC is identified, the pathologist must quantify the tumor components, define the grade of differentiation of the conventional SCC foci, and determine the depth of invasion, as well as evaluate lymphovascular and/or perineural invasion, in order to assist clinicians in determining adjuvante therapeutic options.41
Several therapeutic approaches are employed for oral mucosal VC, including surgery, chemotherapy, and radiotherapy.42
Among the therapeutic options, wide surgical excision is generally considered the treatment of choice, with recommended safety margins of at least 5 mm to minimize the risk of local recurrence.12, 16, 19, 43, 44 Neck dissection is typically not required for VC, as the neoplasm tends to invade locally but rarely metastasizes to lymph nodes.19, 45, 46 In this context, cervical lymphadenopathy associated with VC represents, in most cases, reactive changes rather than metastases.31 In cases involving extensive lesions, surgery may not be feasible and lead to unsatisfactory functional and cosmetic results.16 When resection is not indicated, therapeutic alternatives can be used, such as cytostatic drugs, imiquimod, α-interferon, and oral retinoids.4 The use of high-dose cytostatic agents has shown benefits in reducing VC size, while the complementary use of interferon (IFN) has the potential to slow tumor growth.47 Chemotherapy with bleomycin or methotrexate has demonstrated success, used either as a monotherapy for inoperable cases or as neoadjuvant therapy to reduce the size of extensive lesions prior to surgery.148, 49
Regarding radiotherapy, some studies report the occurrence of radiation-induced anaplastic transformation of VC, which usually manifests 2−8 months after the end of treatment.50, 51 Although the potential for anaplastic transformation remains controversial, radiotherapy is considered a salvage option when surgery is not feasible or when histopathological findings indicate adverse risk features, such as positive lymph nodes or invasion of deeper vital structures (e.g., nerves and blood vessels).8, 13, 52
Regardless of the treatment modality, local recurrence rates are high, ranging from 30% to 50%, with a tendency to recur in the form of less differentiated carcinomas.32 Nevertheless, the prognosis for oral VC is usually favorable compared to other malignant tumors (7−8% mortality rate), except for hybrid carcinoma cases, which carry a worse prognosis and must be managed as conventional SCC.7, 37 The 5-year overall survival rate ranges from 64% to 94%, and the stage at diagnosis is the most relevant prognostic factor.7, 16, 17 In oral VC cases, surgical intervention appears to be related to improved overall survival, whereas advanced age and higher staging are associated with worse overall survival and disease-specific survival rates.53
Furthermore, it is important to distinguish VC from other verrucous lesions, particularly proliferative verrucous leukoplakia and verrucous hyperplasia (VH).38 Proliferative verrucous leukoplakia is an uncommon, progressive form of multifocal leukoplakia characterized by a high rate of malignant transformation to SCC or VC, as well as a significant recurrence rate. Although lesions often begin as simple, flat hyperkeratosis, indistinguishable from conventional leukoplakia, proliferative verrucous leukoplakia presents persistent growth, evolving into exophytic, verrucous forms.38 Thus, current evidence suggests that untreated leukoplakia can progressively evolve into VH and/or VC.11
Clinical distinction between VH and VC is challenging.11 VH is considered an antecedent or early form of VC, and the transition is so consistent that dysplasia, once diagnosed, should be treated as VC.4, 38, 54, 55 Strict clinical monitoring of VH is essential to detect any potential transition to VC.11 The differential diagnosis is established microscopically, but an incisional biopsy must be performed with adequate margins to ensure a correct diagnosis. In VH, the hyperplastic epithelium and verrucous processes are superficial to the adjacent normal epithelium. In contrast, in VC, although the verrucous processes are superficial, the epithelial ridges extend deeply relative to the adjacent normal epithelium.38, 56, 57 Finally, VC must also be differentiated histologically from papillary SCC, which exhibits marked cellular atypia and frank invasion of the basement membrane.7
It is noteworthy that a thorough microscopic examination is essential for the differential diagnosis and appropriate treatment of VC and other verrucous lesions. Santoro et al.31 identified common pitfalls during the evaluation of verrucous lesions: histologically underdiagnosed cases, diagnosed a keratosis or VH, with synchronous or metachronous aggressive growth patterns; clinically undertreated cases, with proliferative verrucous leukoplakia and VC lacking a microscopic diagnosis of epithelial dysplasia; and surgically overtreated cases, including VC managed as conventional SCC, with radical resection and unnecessary lymphadenectomy. Thus, an accurate diagnosis relies on a comprehensive assessment of all characteristics rather than an isolated evaluation of individual findings, and close collaboration between clinicians and pathologists is essential.31
VC is a rare variant of oral SCC characterized by locally invasive and typically non-metastatic behavior, carrying a more favorable prognosis than conventional SCC. The differential diagnosis between VC and other verrucous lesions remains a challenge for pathologists, especially when biopsy specimens are insufficient and inaccurate and obtained from unrepresentative areas. An adequate biopsy from the periphery of the lesion, with sufficient depth and inclusion of adjacente normal tissue, is critical for differential diagnosis and for the analysis of potential areas of cytologic atypia, epitelial dysplasia, and hybrid SCC. Thus, histopathologic distinction is essential for appropriate management, as VC requires more conservative treatment than conventional SCC. In addition, close communication between the clinician and the pathologist is mandatory for a correct diagnosis. Ultimately, the treatment of choice for VC is surgical excision. While the role o radiotherapy remains controversial, some authors suggest it for extensive tumors where surgery is not feasible or for patients with poor general health status.
References
1. Ackerman LV. Verrucous carcinoma of the oral cavity. Surgery. 1948;23:670-8.
2. Koch BB, Trask DK, Hoffman HT, Karnell LH, Robinson RA, Zhen W, et al. National survey of head and neck verrucous carcinoma: patterns of presentation, care, and outcome. Cancer. 2001;92:110-20.
3. Kleihues P, Sobin LH, series eds. World Health Organization Classification of Tumors. Lyon, France: IARC Press, 2005, 168-175.
4. Fakhraei S, Layegh P, Darchini-Maragheh E, Meybodi NT. Oral verrucous carcinoma arising from pemphigus vulgaris: A rare coincidence. Oral Oncol. 2022;124:105513.
5. Pravda C, Srinivasan H, Koteeswaran D, Manohar LA. Verrucous carcinoma in association with oral submucous fibrosis. Indian J Dent Res. 2011;22:615.
6. Rekha KP, Angadi PV. Verrucous carcinoma of the oral cavity: a clinico-pathological appraisal of 133 cases in Indians. Oral Maxillofac Surg. 2010;14:211-8.
7. Zidar N, Cardesa A, Gillison M, Helliwell TR, Hille J, Nadal A. Verrucous squamous cell carcinoma. Pathology and Genetics of Tumors of the Head and Neck. WHO Classification of Tumors, 4th edn. Lyon: IARC, 2017:84-85.
8. Asha ML, Vini K, Chatterjee I, Patil P. Verrucous carcinoma of buccal mucosa: a case report. International Journal of Health Sciences. 2014;1:19-23.
9. Ramani P, Krithika C, Ananthalakshmi R, Singaram M, Jagdish P, Janardhanan S, et al. Verrucoid Variant of Invasive Squamous Cell Carcinoma in Oral Submucous Fibrosis: A Clinicopathological Challenge. Cureus. 2016;8:e862.
10. Chaisuparat R, Limpiwatana S, Kongpanitkul S, Yodsanga S, Jham BC. The Akt/mTOR pathway is activated in verrucous carcinoma of the oral cavity. J Oral Pathol Med. 2016;45:581-5.
11. Alkan A, Bulut E, Gunhan O, Ozden B. Oral verrucous carcinoma: a study of 12 cases. Eur J Dent. 2010;4:202-7.
12. Sadasivan A, Thankappan K, Rajapurkar M, Shetty S, Sreehari S, Iyer S. Verrucous lesions of the oral cavity treated with surgery: Analysis of clinico-pathological features and outcome. Contemp Clin Dent. 2012;3:60-3.
13. Rahali L, Omor Y, Mouden K, Mahdi Y, Elkacemi H, Elmajjaoui S, et al. Oral verrucous carcinoma complicating a repetitive injury by the dental prosthesis: a case report. Pan Afr Med J. 2015;20:297. Published 2015 Mar 26.
14. Depprich, RA, Handschel JG, Fritzemeier CU, Engers R, Kübler NR. Hybrid verrucous carcinoma of the oral cavity: A challenge for the clinician and the pathologist. Oral Oncology Extra. 2006;42:85-90.
15. Oliveira DT, de Moraes RV, Fiamengui Filho JF, Fanton Neto J, Landman G, Kowalski LP. Oral verrucous carcinoma: a retrospective study in São Paulo Region, Brazil. Clin Oral Investig. 2006;10:205-9.
16. Candau-Alvarez A, Dean-Ferrer A, Alamillos-Granados FJ, Heredero-Jung S, Garcia-Garcia B, Ruiz-Masera JJ, et al. Verrucous carcinoma of the oral mucosa: an epidemiological and follow-up study of patients treated with surgery in 5 last years. Med Oral Patol Oral Cir Bucal. 2014;19:e506-11.
17. Alonso JE, Kuan EC, Arshi A, St John MA. A population-based analysis of verrucous carcinoma of the oral cavity. Laryngoscope. 2018;128:393-7.
18. Chung CH, Yang YH, Wang TY, Shieh TY, Warnakulasuriya S. Oral precancerous disorders associated with areca quid chewing, smoking, and alcohol drinking in southern Taiwan. J Oral Pathol Med. 2005;34:460-6.
19. Karagozoglu KH, Buter J, Leemans CR, Rietveld DH, van den Vijfeijken S, van der Waal I. Subset of patients with verrucous carcinoma of the oral cavity who benefit from treatment with methotrexate. Br J Oral Maxillofac Surg. 2012;50:513-8.
20. Walvekar RR, Chaukar DA, Deshpande MS, Pai PS, Chaturvedi P, Kakade A, et al. Verrucous carcinoma of the oral cavity: A clinical and pathological study of 101 cases. Oral Oncol. 2009;45:47-51.
21. Torrejon-Moya A, Jané-Salas E, López-López J. Clinical manifestations of oral proliferative verrucous leukoplakia: a systematic review. J Oral Pathol Med. 2020;49:404-8.
22. Mithani SK, Mydlarz WK, Grumbine FL, Smith IM, Califano JA. Molecular genetics of premalignant oral lesions. Oral Dis. 2007;13:126–33.
23. Warshaw EM, Templeton SF, Washington CV. Verrucous carcinoma occurring in a lesion of oral lichen planus. Cutis. 2000;65:219-22.
24. Greer Jr RO, Eversole LR, Crosby LK. Detection of human papillomavirus-genomic DNA in oral epithelial dysplasias, oral smokeless tobacco-associated leukoplakias, and epithelial malignancies. J Oral Maxillofac Surg. 1990;48:1201-5.
25. Pleat JM, Bradley M, Orlando A, Rigby H. Verrucous carcinoma of the temporal bone: a wolf clothed in wool. Skull Base. 2004;14:39-46.
26. Martin F, Dalac S, Lambert D. Le carcinome verruqueux situation nosologique, a propos de quatre cas. Ann Dermatol Venereol. 1995;122:399-403.
27. Peng Q, Wang Y, Quan H, Li Y, Tang Z. Oral verrucous carcinoma: From multifactorial etiology to diverse treatment regimens (Review). Int J Oncol. 2016;49:59-73.
28. Asproudis I, Gorezis S, Aspiotis M, Tsanoou E, Kitsiou E, MArminga E, et al. Orbital metastasis from verrucous carcinoma of the oral cavity: case report and review of the literature. In Vivo. 2007;21:909-12.
29. Garcia NG, Oliveira DT, Hanemann JA, Pereira AA. Oral verrucous carcinoma mimicking a chronic candidiasis: a case report. Case Rep Oncol Med. 2012;2012:190272.
30. Ghelbazouri NE, Afifi Y, Benameur H, Bella AE, Elhallaoui Y, Kettani F, et al. Oral verruqueux carcinoma and papillomavirus infection. Ann Dermatol Venereol. 2007;134:659-62.
31. Santoro A, Pannone G, Contaldo M, Sanguedolce F, Esposito V, Serpico R, et al. A troubling diagnosis of verrucous squamous cell carcinoma (“the bad kind” of keratosis) and the need for clinical and pathological correlations: a review of the literature with a case report. J Ski Cancer. 2011;2011:370605.
32. Alan H, Agacayak S, Kavak G, Ozcan A. Verrucous carcinoma and squamous cell papilloma of the oral cavity: Report of two cases and review of literature. Eur J Dent. 2015;9:453-6.
33. Waskowska J, Koszowski R, Raczkowska-Siostrzonek A, Stemplewska K. Verrucous carcinoma of the tongue-a rare case study. Cent Eur J Med. 2012;7:145–8.
34. Woolgar JA, Triantafyllou A. Pitfalls and procedures in the histopathological diagnosis of oral and oropharyngeal squamous cell carcinoma and a review of the role of pathology in prognosis. Oral Oncol. 2009;45:361-85.
35. Mehrotra D, Goel M, Kumar S, Pandey R, Ram H. Oral verrucous lesions: Controversies in diagnosis and management. J Oral Biol Craniofac Res. 2012;2:163-9.
36. Piemonte ED, Lazos PJ, Brunotto M. Relationship between chronic trauma of the oral mucosa, oral potentially malignant disorders and oral cancer. J Oral Pathol Med. 2010;39:513-7.
37. Iriarte-Ortabe J, Laka A, Marbaix E, Reychler H. Le carcinome verruqueux buccal: analyse de 6 cas cliniques et revue de la littérature. Journal Français d’Oto-rhino-laryngologie. 1991;40:404-3.
38. Komal K, Deshmukh SB, Deshmukh A. Verrucous Carcinoma with Oral Submucous Fibrosis: A Rare Case with Brief Review. J Clin of Diagn Res. 2015;9:ED06-8.
39. Terada T. Verrucous carcinoma of the oral cavity: a histopathologic study of 10 Japanese cases. J Maxillofac Oral Surg. 2011;10:148-51.
40. Gokavarapu S, Rao LMC, Patnaik SC, Parvataneni N, Raju KVVN, Chander R, et al. Reliability of Incision Biopsy for Diagnosis of Oral Verrucous Carcinoma: A Multivariate Clinicopathological Study. J Maxillofac Oral Surg. 2015;14:599-604.
41. Devaney KO, Ferlito A, Rinaldo A, El-Naggar AK, Barnes L. Verrucous carcinoma (carcinoma cuniculatum) of the head and neck: what do we know now that we did not know a decade ago? Eur Arch Otorhinolaryngol. 2011;268:477-80.
42. Kristofelc N, Zidar N, Strojan P. Oral verrucous carcinoma: a diagnostic and therapeutic challenge. Radiol Oncol. 2023;57:1-11. PMID: 36942907; PMCID: PMC10039467.
43. Rath S, Gandhi AK, Rastogi M, Agarwal A, Singhal A, Sharma V, et al. Treatment Pattern and Outcomes in Verrucous Carcinoma of Oral Cavity: A Single Institutional Retrospective Analysis from a Tertiary Cancer Center and Review of Literature. Indian J Otolaryngol Head Neck Surg. 2022;74(Suppl 2):1790-6.
44. Verma DK, Bansal S, Gupta D, Bansal A. Neck dissection in verrucous carcinoma: A surgical dilemma. IJSS Case Rep Ver 2015;1:42-5.
45. Ferlito A, Recher G. Ackerman’s tumor (verrucous carcinoma) of the larynx: a clinicopathologic study of 77 cases. Cancer. 1980;46:1617-30.
46. Kato A, Takahashı Y, Yanohara K. Verrucous carcinoma of the tongue; a case report. Pract Otorhinolaryngol. 1991;84:775-80.
47. Risse L, Negrier P, Dang PM, Bedane C, Bernard P, Labrousse F, et al. Treatment of verrucous carcinoma with recombinante alpha-interferon. Dermatology. 1995;190:142-4.
48. Jyothirmayi R, Sankaranarayanan R, Varghese C, Jacob R, Nair MK. Radiotherapy in the treatment of verrucous carcinoma of the oral cavity. Oral Oncol. 1997;33:124-8.
49. Kamath VV, Varma RR, Gadewar DR, Muralidhar M. Oral verrucous carcinoma. An analysis of 37 cases. J Craniomaxillofac Surg. 1989;17:309-14.
50. Batsakis JG, Hybels R, Crissman JD, Rice DH. The pathology of head and neck tumors: verrucous carcinoma, Part 15. Head Neck Surg. 1982;5:29-38.
51. Tharp ME 2nd, Shidnia H. Radiotherapy in the treatment of verrucous carcinoma of the head and neck. Laryngoscope. 1995;105(4Pt1):391-6.
52. McClure DL, Gullane PJ, Slinger RP, Wysocki GP. Verrucous carcinoma-changing concepts in management. J Otolaryngol. 1984;13:7-12.
53. Alonso JE, Han AY, Kuan EC, Suh JD, St John MA. Epidemiology and survival outcomes of sinonasal verrucous carcinoma in the United States. Laryngoscope. 2018;128:651-6.
54. Seymour RA, Thomason JM, Nolan A. Oral lesions in organ transplant patients. J Oral Pathol Med. 1997;26:297-304.
55. Ko MJ, Chu CY. Disseminated human papillomavirus type 11 infection in a patient with pemphigus vulgaris: confirmed by DNA analysis. J Am Acad Dermatol. 2004;51(5 Suppl):S190-3.
56. Akrish S, Eskander-Hashoul L, Rachmiel A, Ben-Izhak O. Clinicopathologic analysis of verrucous hyperplasia, verrucous carcinoma and squamous cell carcinoma as part of the clinicopathologic spectrum of oral proliferative verrucous leukoplakia: A literature review and analysis. Pathol Res Pract. 2019;215:152670.
57. Shear M, Pindborg JJ. Verrucous hyperplasia of the oral mucosa. Cancer. 1980;46:1855-62.
Josivaldo Bezerra Soares
E-mail address: josivaldo.soares@academico.ufpb.br
CRediT authorship contribution statement
Josivaldo Bezerra Soares: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing. Beatriz Medeiros Batista: Investigation, Visualization, Writing – original draft, Writing – review & editing. Sérgio Cantídio Carneiro Morais: Visualization, Writing – original draft, Writing – review & editing. Cícera Dalylla Lopes Ferreira: Visualization, Writing – original draft, Writing – review & editing. Katia Caetana Pereira: Visualization, Writing – original draft, Writing – review & editing. Paulo Rogério Ferreti Bonan: Conceptualization, Visualization, Supervision, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
1646-2890/© 2026 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).