
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2025 | 66 (4) | 199-206
Original research
Does cavity disinfection affect the bond strength between Biodentine or mineral trioxide aggregate and a glass ionomer cement? – An in vitro study
A desinfeção da cavidade afeta a resistência de união entre a Biodentine ou o agregado trióxido mineral e um cimento de ionómero de vidro? – Um estudo in vitro
a Department of Endodontics, Faculty of Dentistry, Antalya Bilim University, Antalya, Turkiye
b Department of Endodontics, Faculty of Dentistry, Akdeniz University, Antalya, Turkiye
Deniz Yanik Nalbanto?lu - deniz.yanik@yahoo.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 66
Issue - 4
Original research
Pages - 199-206
Go to Volume
Article History
Received on 15/11/2024
Accepted on 14/12/2025
Available Online on 30/12/2025
Keywords
Original Research
Does cavity disinfection affect the bond strength between Biodentine or mineral trioxide aggregate and a glass ionomer cement? – An in vitro study
A desinfeção da cavidade afeta a resistência de união entre a Biodentine ou o agregado trióxido mineral e um cimento de ionómero de vidro? – Um estudo in vitro
Deniz Yanık Nalbantoğlu1 0000-0001-5676-0293
Kürşat Er2 0000-0002-0667-4909
Alper Kuştarcı2 0000-0002-4942-3739
1 Department of Endodontics, Faculty of Dentistry, Antalya Bilim University, Antalya, Turkiye.
2 Department of Endodontics, Faculty of Dentistry, Akdeniz University, Antalya, Turkiye.
Article history:
Received 15 November 2024
Accepted 14 December 2025
Available online 31 December 2025
Abstract
Objectives: The study aims to evaluate the influence of cavity disinfectants on the shear bond strength between Biodentine and mineral trioxide aggregate (MTA) associated with conventional glass ionomer (GIC) or resin-modified glass ionomer (RMGIC).
Methods: For the study, 144 acrylic mounts were prepared and divided into four groups: MTA-GIC, MTA-RMGIC, Biodentine-GIC, and Biodentine-RMGIC. These were further divided into cavity disinfectant subgroups: sodium hypochlorite (NaOCl), chlorhexidine, and control. Glass ionomers were applied to the silicate cements after performing cavity disinfection. Shear bond strength was analyzed. For statistical analysis, Student’s t-test and one-way ANOVA were used.
Results: RMGIC showed lower shear bond strength values to MTA and Biodentine than CGIC in all subgroups (P < 0.05). The shear bond values were lower in chlorhexidine than in NaOCl and control groups (P < 0.05). Biodentine and MTA had statistically similar shear bond values to the glass ionomer cements (P > 0.05). The failure types were 38.88% adhesive, 30.55% mixed, and 30.55% cohesive.
Conclusions: GIC bonded more strongly to MTA and Biodentine than RMGIC. MTA and Biodentine bonded similarly to glass ionomers. Chlorhexidine decreased bond strength, while NaOCl did not. (Rev Port Estomatol Med Dent Cir Maxilofac. 2025;66(4):199-206)
Keywords: Adhesion, Biodentine,Cavity disinfectant, Glass ionomer cements, Mineral trioxide aggregate, Shear strength
Resumo
Objetivos: O objetivo deste estudo foi avaliar a influência dos desinfetantes de cavidade na resistência de união ao cisalhamento (RUC) entre Biodentine e agregado de trióxido mineral (MTA) associados a cimento de ionómero de vidro convencional (CIVCC) ou cimento de ionómero de vidro modificado por resina (CIVMR).
Métodos: Foram preparadas 144 restaurações acrílicas para o estudo, divididas em quatro grupos: MTA-CIVCC, MTA-CIVMR, Biodentine- CIVCC e Biodentine-CIVMR. Estes foram divididos em subgrupos de desinfetantes da cavidade: hipoclorito de sódio (NaOCl), clorexidina e controlo. Os ionómeros de vidro foram aplicados nos cimentos de silicato após a desinfeção da cavidade. A RUC foi analisada. O teste t de Student e a ANOVA unidirecional foram utilizados para a análise estatística.
Resultados: O CIVMR mostrou valores de RUC mais baixos com o MTA e o Biodentine do que o CIVCC em todos os subgrupos (P < 0,05). Os valores de RUC foram mais baixos no grupo tratado com clorohexidina do que nos grupos tratados com NaOCl e no grupo controlo (P < 0,05). O Biodentine e o MTA obtiveram valores de RUC estatisticamente semelhantes quando associados aos cimentos de ionómero de vidro (P > 0,05). Os tipos de falha foram 38,88% adesivas, 30,55% mistas e 30,55% coesivas.
Conclusões: O CIVCC apresentou maior resistência de união ao MTA e ao Biodentine do que o CIVMR. O MTA e o Biodentine apresentaram uma resistência de união semelhante com os ionómeros de vidro. A clorohexidina diminuiu a resistência de união, enquanto o NaOCl não apresentou este efeito.
Palavras-chave: Adesão, Biodentine,Desinfetante cavitário,Cimentos de ionómero de vidro,Agregado de trióxido mineral, Resistência ao cisalhamento
Introduction
Vital pulp treatment strategies offer valuable options for protecting dental pulp with strong regeneration potential. Restorative materials used in vital pulp therapies should be highly biocompatible, low in cytotoxicity, and bioactive.1, 2 Calcium silicate cements are well-established and comprehensively used in dentistry, especially in regenerative procedures, vital pulp therapies, repairing perforations, and root-end filling.
Mineral trioxide aggregate (MTA) is the precursor of silicate- based cements and is considered the gold standard, having been comprehensively analyzed in the literature.3 - 6 However, MTA drawbacks and technological developments led to the pursuit of a more optimum material among various types of silicate-based cement with different mechanical or biological properties.5, 6 One alternative is Biodentine, which is a fast-setting silicate-based cement composed of a powder that includes tricalcium silicate and a liquid that includes a hydrosoluble polymer and calcium chloride for acceleration.7, 8
The coronal seal, crucial for any restoration, is highly affected by the cohesive resistance of the restorative materials and by the bond strength between them.3, 5The quality of a coronal seal depends on the material’s mechanical properties and the adhesion both to the dentin and between the diferente restorative materials used.5,7 In spite of their beneficial biological properties, using calcium silicate cements as a base restorative material is impractical due to improper compressive or flexural strength and cohesive resistance.9 To maintain the structural integrity of the restoration under the occlusal forces, a more resistant material with a better cohesive strength is required as a cavity liner.
Glass ionomer cement (GIC) is very popular in dentistry as a cavity liner and is known for its anti-caries properties with fluoride release.10, 11 GIC’s chemical bonding to dentin and the fact that it does not irritate the pulp-dentin complex prominently support its preference as a cavity liner. Resin-modified glass ionomer cements (RMGIC) contain similar contents to conventional GIC, but incorporate monomers, and their setting mechanism involves both polymerization and an acid-base reaction.11 Due to its mechanical properties, RMGIC does not require a strong compaction force during placement in the cavity, which is beneficial for the stability of a perforation repair material.3, 4
In the presence of bacteria, dentin degrades, potentially leading to secondary caries and restoration failure.12 Therefore, microbial control with cavity disinfectants is one of the crucial stages of the restorative procedures. Numerous chemicals are used as cavity disinfectants, and different types of lasers or ozone have also been reported as cavity disinfection methods.3, 12, 13 Chlorhexidine gluconate, a very commonly used cavity disinfectant, is a biguanide with a desirable bacterial spectrum of action and favorable properties, including substantivity and inhibition of matrix metalloproteinases. However, its influence on bond strength is still controversial.12, 14 In turn, sodium hypochlorite (NaOCl) is a very effective and easyto-use agent. As a cavity disinfectant, it is used in 0.5% and 10% concentrations.12, 15 After perforation repair, it is used as a cavity disinfectant or root canal irrigant, and frequently interacts with silicate-based cement. Using a cavity disinfectant may vary the wettability or bond strength of both dentin and the materials themselves.16 When a cavity with a perforation that was restored with a repair material is disinfected, the chemical structure of the cavity disinfectant can affect the repair material negatively.3, 6, 12 Although only a minor part of all bonded surfaces of the cavity fails, it dislodges the restoration and compromises the success. Therefore, understanding the effect of cavity disinfectants on shear bond strength has clinical importance.
The objective of the study is to compare the shear bond strength between conventional GIC or RMGIC and MTA or Biodentine with the application of NaOCl and chlorhexidine.
Material and Methods
One hundred forty-four acrylic blocks with a round hole located at the center, 2 mm deep and 4 mm in diameter, were prepared for the study in cylindrical form. The study groups are shown in Figure 1. The samples were divided into two groups according to the perforation repair material (n=72): MTA (MTA Angelus; Angelus, Londrina, PR, Brazil) and Biodentine (Septodont, Saint-Maur-des-Fosses, France). Table 1 indicates the composition and manufacturers of materials used in this study. MTA and Biodentine were prepared according to the manufacturer’s instructions. The samples’ holes were filled with cement using a spatula and covered with a moist cotton pellet. To ensure proper cement setting, the samples were stored at 100% humidity at 37°C. According to the manufacturer’s instructions, the moist cotton pellet was applied to the silicate cement during a 15-minute setting time.
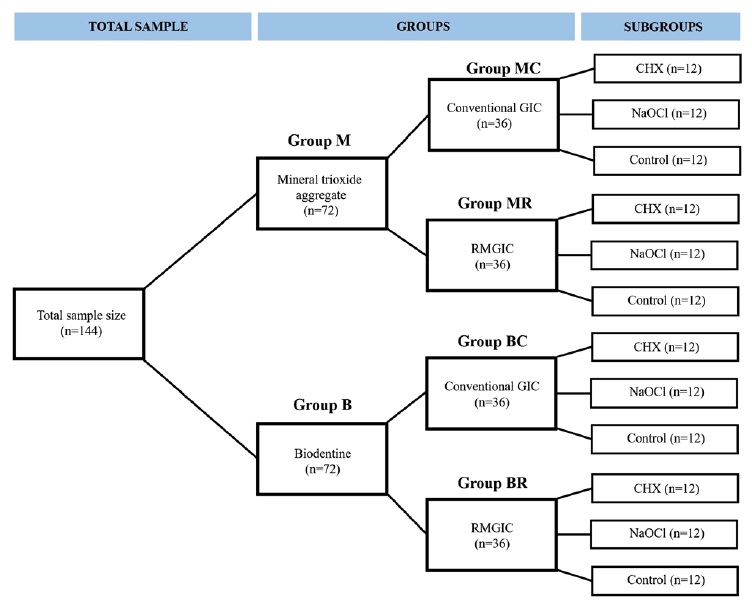
Figure 1. The sample size and the groups of the study (GIC – Glass ionomer cement; CGIC – Conventional GIC;
RMGIC – Resin-modified GIC; NaOCl – Sodium hypochloride; CHX – Chlorhexidine gluconate).
After the 15-minute setting time,17 the sample groups were divided into four groups according to the materials to be used (n=36): MTA + conventional GIC, Biodentine + conventional GIC, MTA + RMGIC, and Biodentine + RMGIC. Each of these groups was further divided into three subgroups based on the cavity disinfectant used (n=12): chlorhexidine, NaOCl, and control. In the chlorhexidine subgroup, 2% chlorhexidine (Klorhex, Drogsan, Istanbul, Turkiye) was applied with an injector for 1 min; subsequently, the surface was gently dried with air pressure.
In the NaOCl subgroup, 5.25% NaOCl was applied similarly to chlorhexidine and then dried. In the control group, GIC was applied directly without applying any disinfectant. Until the cavity disinfectant was applied, the samples were kept at 37°C and 100% humidity, and the moist cotton pellets were renewed to prevent drying out.
After cavity disinfection procedures were performed, conventional GIC and RMGIC were placed using a 4 mm-high, 3 mm-diameter plastic tube on MTA and Biodentine. Conventional GIC (Fuji IX; GC, Tokyo, Japan) was mixed according to the manufacturer’s instructions, packed into plastic tubes, and compacted to hamper air trapping. RMGIC (Ionoseal; Voco, Germany) was applied incrementally using its syringe into plastic tubes, and each layer was polymerized (Elipar DeepCure-S; 3M ESPE, Seefeld, Germany) at 400 mW/cm2 for 40 sec. After polymerization, the plastic tubes were carefully removed, and the samples were stored for 24 h at 37 °C and 100% humidity.6
Shear bond strength was measured using a universal testing machine (Instron, AGS-1000Kgw®; Shimadzu Corp., Chiroda-Ku, Tokyo, Japan) with a knife-edge blade. A crosshead speed of 0.5 mm/min was applied to each sample until failure occurred between the two materials. The values were recorded in Newton (N) using the Trapezium X Software (Shimadzu, Kyoto, Japan) and converted to megapascal (MPa). Calculations were made with this formula: maximum load/sample surfasse area (πr2). – Failure was classified into three types: adhesive failure between two different materials; cohesive failure within a single material; and mixed failure, which combined adhesive and cohesive failure.
Statistical analyses were carried out using SPSS version 26.0 for Windows (IBM Corp., Armonk, NY, USA). Shapiro-Wilk and Levene’s tests were used to analyze the normality and homogeneity of the data. One-way ANOVA and post hoc Tukey tests were used to analyze the differences between the cavity disinfection method subgroups, and Student’s t-test was used to compare MTA and Biodentine. The statistical significance was set at P < 0.05 with a 95% confidence interval.
Results
The descriptive analysis, mean, maximum, minimum, and standard deviation are demonstrated in Tables 1 and 2. The mean shear bond strength values between MTA and conventional GIC and RMGIC were 4.75−6.84 MPa and 3.67−4.89 MPa, respectively. The Student’s t-test revealed a significant difference in bond strength between the MTA–conventional GIC interface and the MTA–RMGIC interface (P < 0.05). Shear bond strength was lower in the MTA–RMGIC interface than in the MTA–conventional GIC interface in all subgroups (P < 0.05). Similar results were observed in shear bond to Biodentine: it was lower at the Biodentine–RMGIC interface than at the Biodentine–conventional GIC interface in all subgroups (P < 0.05).
Table 1. Restoration materials used in the study.
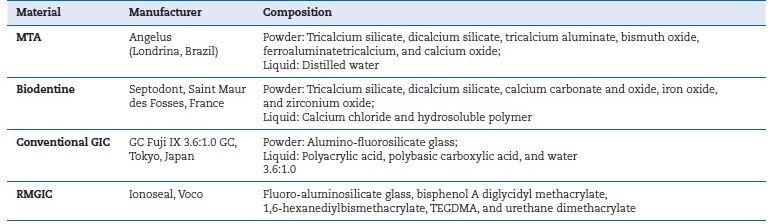
MTA – Mineral trioxide aggregate; GIC – Glass ionomer cement; CGIC – Conventional GIC; RMGIC – Resin-modified GIC;
NaOCl – Sodium hypochloride; CHX – Chlorhexidine gluconate
Table 2. Shear bond strength values in different cavity disinfectants according to the tricalcium silicate cement.
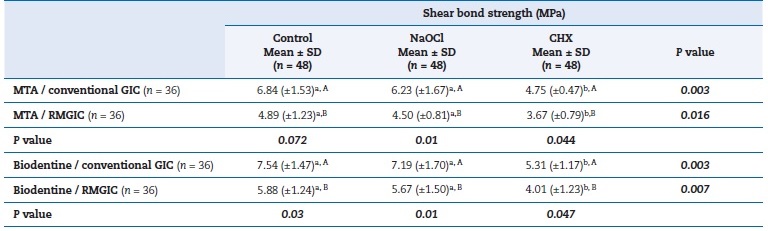
MTA – Mineral trioxide aggregate; GIC – Glass ionomer cement; RMGIC – Resin-modified GIC; NaOCl– Sodium hypochlorite;
CHX – Chlorhexidine gluconate
Different lowercase superscripts in the row indicate statistical differences according to one-way ANOVA (P < 0.05). Different uppercase superscripts in the column indicate statistical differences according to Student’s t-test (P < 0.05). Bold p values indicate statistical difference.
SD – Standard deviation.
The mean shear bond strength values at the Biodentine–conventional GIC and the Biodentine–RMGIC interfaces were 5.31−7.54 MPa and 4.01−5.88 MPa, respectively. The bond strengths of conventional GIC were similar to MTA and Bio dentine. Similarly, there were no statistical difference between the bond strength values of RMGIC to MTA and Biodentine (Figure 2).
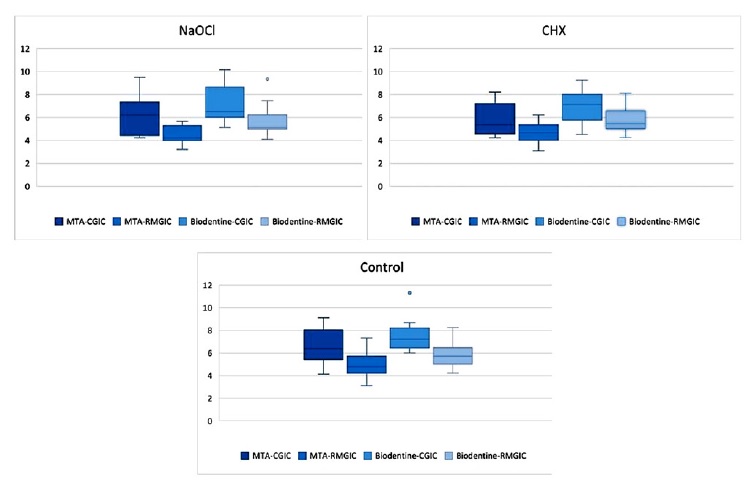
Figure 2. The bond strength values of the study groups.
Regarding subgroups, there was a statistically significant difference in the bond strength of chlorhexidine subgroups (P < 0.05). According to one-way ANOVA and the post hoc Tukey test, the shear bond strength values were lower in the chlorhexidine subgroups than the control and NaOCl subgroups (P < 0.05). There was no statistical difference between the control and NaOCl subgroups (Table 3).
Table 3. Shear bond strength values in different cavity disinfectants according to the GIC types.
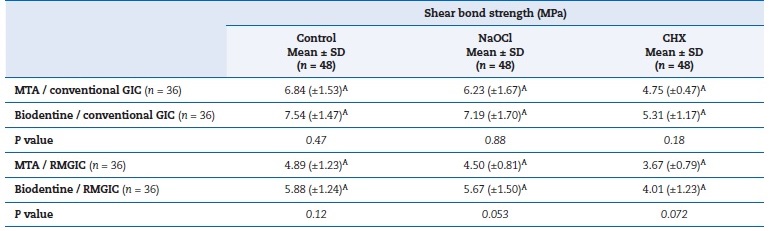
MTA – Mineral trioxide aggregate; GIC – Glass ionomer cement; RMGIC – Resin-modified GIC; NaOCl – Sodium hypochlorite;
CHX – Chlorhexidine gluconate
Different uppercase superscripts in the column indicate statistical differences according to Student’s t-test (P < 0.05). Bold p values indicate
statistical difference. SD – Standard deviation.
The failure types are shown in Table 4. The percentages of failure types in the MTA–conventional GIC interface were 41.66%, 27.77%, and 30.55% for adhesive, mixed, and cohesive, respectively. For the MTA–RMGIC interface, these values were 36.11%, 36.11%, and 27.77%, respectively. The failure types at the Biodentine–conventional GIC interface were 44.44%, 27.77%, and 27.77% for adhesive, mixed, and cohesive, respectively, and at the Biodentine–RMGIC interface were 33.33%, 30.55%, and 36.11%, respectively.
Table 4. Failure types according to the study groups.
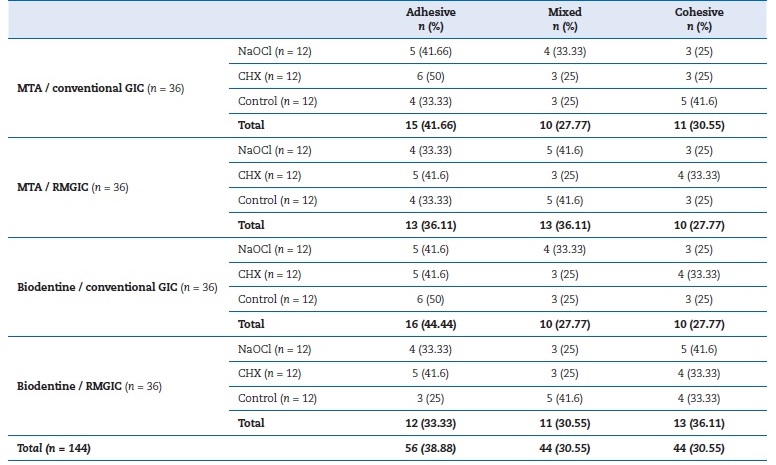
MTA – Mineral trioxide aggregate; GIC – Glass ionomer cement; RMGIC – Resin-modified GIC; NaOCl – Sodium hypochlorite;
CHX – Chlorhexidine gluconate
Discussion
In this study, MTA and Biodentine were similarly bound to glass ionomers. It was also shown that the bond strength of conventional GIC to MTA and Biodentine was higher than that of RMGIC. According to the results, the bond strength between MTA and conventional GIC was 6.84 MPa. In the literature, this bond strength was not investigated comprehensively, but the few studies found reported values between 5, 8 and 8.85 MPa.18, 19 In turn, bond strength values between MTA and RMGIC reported in the literature range from 1.7 to 7.58 MPa,3, 6, 9, 17 which agrees with the 4.89 MPa value found in our study. When comparing GIC types, conventional GIC bonded more strongly to the MTA than RMGIC. The lower bond strength values observed in RMGIC can be attributed to the presence of an unpolymerized monomer on the bonding surfasse with silicate cement, as this cement is polymerized via light curing. Therefore, in cases where the bond strength is compromised, conventional GIC may be preferred over RMGIC when bonding to MTA to obtain a more stable restoration.
There is limited data about the bond strength between Biodentine and conventional GIC. A previous study19 reported a value of 6.7 MPa, which is slightly lower than our result of 7.54 MPa. Another study7 reported a bond strength of 0.80 MPa between Biodentine and conventional GIC. This bond strength is considerably lower than that reported in our findings. This difference may be due to the lack of standardization in GIC’s mixing procedure.
Our results revealed a shear bond strength between Biodentine and RMGIC of 5.88 MPa, which is the highest in the literature, where bond strength values vary between 1.13 and 5.05 MPa.3, 7, 17 Conventional GIC bonded strongly to Biodentine compared to RMGIC. As with MTA, conventional GIC could be the first option for better bonding as a liner over silicate cement. The better the bond strength, the stronger the coronal seal.
In the present study, GIC was used as a lining material instead of a direct composite restoration. The rinsing procedures used during selective etching for composite filling may dislodge the silicate cement. Although the bond strength of composites to silicate-based cement was reported to be good,7, 8the application procedures may be negatively affected during single-visit restoration. In the scenario of perforation repair and pulp capping with a silicate-based cement, GIC is already a well-established restorative material. A previous study reported that the conventional form bonded better to Biodentine than the resin-modified form.7 In our study, the conventional form presented a better bond strength to both MTA and Biodentine. However, our results showed that the highest shear bond strength between the silicate-based cement and the restorative material was in the Biodentine–conventional GIC interface. On the other hand, it is important to note that the packing force during the application of conventional GIC may affect the stability of silicate cement, especially shortly after application. Conversely, RMGIC does not require packing or compaction forces; it is only injected into the cavity with a minimum force.
There was no difference in the bond strength to MTA and Biodentine. In contrast to our results, studies have reported lower bond strength at the MTA–RMGIC interface than at the Biodentine–RMGIC interface.6, 19 MTA and Biodentine were launched in the market, targeting similar application areas and sharing a similar chemical composition. Nevertheless, there is a nuance in the liquids of the materials: MTA’s liquid contains only distilled water, while Biodentine’s liquid has calcium chloride and a hydrophilic monomer. Hydrophilic materials reduce the amount of water present, which can increase bond strength.6, 20 However, this possible effect was not reflected at the macro level, as our results showed no difference between Biodentine and MTA.
Bond strength represents interfacial adhesion between two materials. In the presence of bond failure, fractures may occur between two different materials, within the same material, or in a combination of these scenarios. In the in vitro design of the study, the filling material was applied to silicate cement as a cylinder. It was not surrounded by another material or dentin tissue itself, but by emptiness. However, in clinical conditions, the filling material is located in the cavity and supported by the dentin itself. Thus, the results of the study may be lower than clinical values. In this study, cohesive failure was the most frequent type, accounting for 38.88% of failures.
In a previous study, most failures observed were cohesive.6, 9 According to the literature, the higher the cohesive failure, the greater the bond strength.6, 9, 12
For easier and faster clinical treatment, the application time of a lining agent is important and should be as short as possible. However, the structural integrity and stability of the silicate-based cement may need a longer setting time. According to the literature, the final setting may take up to 21 days.
In a previous report, the setting time (3 min, 15 min, and 2 days) did not present any difference in the shear bond strength of MTA and Biodentine.17 In addition to the result, considering the manufacturer’s instructions, we determined the lining material application time as 15 min to mimic the single-visit clinical scenario. Nevertheless, in clinical conditions, the restoration is subjected to occlusal forces immediately after the application. In the present study, shear bond strength forces were performed 24 h later; therefore, the cohesive failures can also be related to the final setting time.
In the clinic, when the silicate-based cement is applied to a perforation or used as a pulp-capping agent, the setting occurs under the moist conditions of tissue fluid. In our study, we used an acrylic block to hold MTA to simulate one-sided moisture conditions. Since the literature found lower flexural strength with one-sided moisture than with two-sided moisture, the one-sided moisture in MTA would affect our results.4 However, we analyzed the shear bond strength, and our failure modes were mostly adhesive. To mitigate this limitation, we renewed the moist cotton and maintained sufficient moisture to promote the setting of silicate-based cement.
In terms of cavity disinfectants, NaOCl did not reduce the bond strength between any of the materials used in our study, whereas chlorhexidine diminished it. Thus, the third null hypothesis that NaOCl and chlorhexidine would not reduce the shear bond strength between GIC and tricalcium cement was partially accepted. Coherently, a previous report by the same authors of the present study demonstrated that chlorhexidine reduced the bond strength between MTA and RMGIC.3 The fact that chlorhexidine reduces the bond strength can be explained by inhibiting crystal formation and causing the occurrence of a flatter silicate cement surface.21 For cavity disinfection, Na-OCl is recommended for better bond strength, especially in a compromised tooth substance.
This in vitro study fails to simulate clinical conditions. Although in vitro studies are often viewed with skepticism, they are also an important part of science and the first step on the long path to achieving optimal results. Further clinical studies are needed to understand the bond strength between silicate-based cements and GICs. Because this study is insuficiente to accurately reflect clinical conditions, the results should be interpreted with caution. It should be noted that due to the presence of numerous complex parameters in the clinical conditions, the results cannot be generalized. Additionally, this study used conventional GIC and RMGIC, so results will differ with a composite or other restorative material. Furthermore, due to the differences in the chemical structure of bioceramic materials, the results of this study cannot be generalized to all MTA brands.
A strength of this study is that it demonstrates the interactions between silicate-based cements and cavity disinfection methods under standardized conditions. Many silicate-based cements and cavity disinfection methods might be preferred in the clinic, and the results of this study can guide clinicians in selecting the appropriate material and cavity disinfection method. However, the results should be replicated and supported by further studies.
Conclusions
According to the results, Biodentine and MTA were similarly bonded to GICs. Conventional GIC adhered to silicate-based cement better than RMGIC. Chlorhexidine reduced the bond strength, while NaOCl did not.
References
1. Amin LE, Montaser M. Comparative evaluation of pulpal repair after direct pulp capping using stem cell therapy and biodentine: an animal study. Aust Endod J. 2021;47:11-9.
2. Silva EJNL, Senna PM, De-Deus G, Zaia AA. Cytocompatibility of Biodentine using a three-dimensional cell culture model. Int Endod J. 2016;49:574-80.
3. Yanık D, Er K, Kuştarci A. Shear bond strength of resinmodified glass ionomer cement bound to mineral trioxide aggregate after various disinfection protocols. Aust Endod J. 2023;49:159-64.
4. Walker MP, Diliberto A, Lee C. Effect of setting conditions on mineral trioxide aggregate flexural strength. J Endod. 2006;32:334-6.
5. Shin JH, Jang JH, Park SH, Kim E. Effect of mineral trioxide aggregate surface treatments on morphology and bond strength to composite resin. J Endod. 2014;40:1210-6.
6. Zarean P, Roozbeh R, Zarean P, Jahromi MZ, Broujeni PM. In vitro comparison of shear bond strength of a flowable composite resin and a single-component glass-ionomer to three diferente pulp-capping agents. Dent Med Probl. 2019;56:239-44.
7. Kenchappa M, Nagaveni NB, Kashetty B. Evaluation of the shear bond strength of methacrylate-based composite, resin-modified glass ionomer cement, and Fuji IX glass ionomer cement with Biodentine as a base. CODS J Dent. 2021;11:40-3.
8. Odabaş ME, Bani M, Tirali RE. Shear bond strengths of different adhesive systems to Biodentine. Sci World J. 2013;10:626103.
9. Gulati S, Shenoy VU, Margasahayam SV. Comparison of shear bond strength of resin-modified glass ionomer to conditioned and unconditioned mineral trioxide aggregate surface: an in vitro study. J Conserv Dent. 2014;17:440-3.
10. Nicholson JW, Sidhu SK, Czarnecka B. Enhancing the mechanical properties of glass-ionomer dental cements: a review. Materials (Basel). 2020;13:2510.
11. Alaohali A, Brauer DS, Gentleman E, Sharpe PT. A modified glass ionomer cement to mediate dentine repair. Dent Mater. 2021;37:1307-15.
12. Coelho A, Amaro I, Rascão B, Marcelino I, Paula A, Saraiva J, et al. Effect of cavity disinfectants on dentin bond strength and clinical success of composite restorations-a systematic review of in vitro, in situ and clinical studies. Int J Mol Sci. 2020;31;22:353.
13. Pinna R, Maioli M, Eramo S, Mura I, Milia E. Carious affected dentine: its behaviour in adhesive bonding. Aust Dent J. 2015;60:276-93.
14. Zhang X, Wang L, Liu S, Bai H, Niu W. Evaluation of the bond strength of chlorhexidine incorporated into the adhesive system composition: A PRISMA guided meta-analysis. J Dent Sci. 2020;15:315-28.
15. Wang J, Song W, Zhu L, Wei X. A comparative study of the microtensile bond strength and microstructural differences between sclerotic and Normal dentine after surfasse pretreatment. BMC Oral Health, 2019;19:1-10.
16. Nima G, Cavalli V, Bacelar-Sá R, Ambrosano GM, Giannini M. Effects of sodium hypochlorite as dentin deproteinizing agent and aging media on bond strength of two conventional adhesives. Microsc Res Tech. 2020;83:186-95.
17. Schmidt A, Schäfer E, Dammaschke T. Shear bond strength of lining materials to calcium-silicate cements at different time intervals. J Adhes Dent. 2017;19:129-35.
18. Yesilyurt C, Yildirim T, Taşdemir T, Kusgoz A. Shear bond strength of conventional glass ionomer cements bound to mineral trioxide aggregate. J Endod. 2009;35:1381-3.
19. Cantekin K, Avci S. Evaluation of shear bond strength of two resin-based composites and glass ionomer cement to puré tricalcium silicate-based cement (Biodentine). J Appl Oral Sci. 2014;22:302-6.
20. Bortoluzzi EA, Broon NJ, Bramante CM, Felippe WT, Tanomaru Filho M, Esberard RM. The influence of calcium chloride on the setting time, solubility, disintegration, and pH of mineral trioxide aggregate and white Portland cement with a radiopacifier. J Endod. 2009;35:550-4.
21. Hong ST, Bae KS, Baek SH, Kum KY, Shon WJ, Lee W. Effects of root canal irrigants on the push-out strength and hydration behavior of accelerated mineral trioxide aggregate in its early setting phase. J Endod. 2010;36:1995-9.
Deniz Yanık Nalbantoglu
E-mail address: deniz.yanik@yahoo.com
CRediT authorship contribution statement
Deniz Yanık Nalbantoğlu: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. Kürşat Er: Validation, Writing – review & editing. Alper Kuştarcı: Validation, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
1646-2890/© 2025 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).