
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2026 | 67 (1) | 21-26
Clinical case
Unusual case of pleomorphic adenoma in the accessory parotid gland
Caso incomum de adenoma pleomórfico na glândula parótida acessória
a Post Graduation Program in Health Science, Federal University of Ceará, Sobral, Brazil
b School of Dentistry, Federal University of Ceara, Brazil
João Vitor Freitas da Silva - onevitor@alu.ufc.br
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 67
Issue - 1
Clinical case
Pages - 21-26
Go to Volume
Article History
Received on 10/03/2025
Accepted on 14/12/2025
Available Online on 30/12/2025
Keywords
Clinical Case Report
Unusual case of pleomorphic adenoma in the accessory parotid gland
Caso incomum de adenoma pleomórfico na glândula parótida acessória
Ivana de Sousa Brandão1 0000-0002-6380-6648
João Vitor Freitas da Silva2,* 0009-0001-5595-6232
Filipe Nobre Chaves1 0000-0001-6345-8156
Marcelo Bonifácio da Silva Sampieri1 0000-0001-7942-6642
Denise Hélen Imaculada Pereira de Oliveira1 0000-0001-6020-2374
1 Post Graduation Program in Health Science, Federal University of Ceará, Sobral, Brazil
2 School of Dentistry, Federal University of Ceara, Brazil
Article history:
Received 10 March 2025
Accepted 14 December 2025
Available online 31 December 2025
Abstract
Pleomorphic adenoma is the most common benign lesion of the salivary glands, primarily affecting the parotid gland. The accessory parotid gland is a salivary tissue separate from the parotid gland, considered an anatomical variation with a low incidence and rarely affected by tumors. A 20-year old female patient presented with a complaint of an increased volume swelling for approximately 18 months. Clinical examination revealed a mobile nodule in the buccal mucosa, palpable intra and extraorally, of firm consistency, asymptomatic, with well-circumscribed contours, and without associated lymphadenopathy. Ultrasonography revealed a rounded hypoechoic image, without associated vascularization, in the angle region of the left mandible. In view of this condition, an excisional biopsy of the lesion was performed under local anesthesia in an outpatient setting. In the intraoperative period, a nodular encapsulated lesion was observed, whose location suggested origin from the accessory parotid gland. Histopathologic analysis confirmed the diagnosis of pleomorphic adenoma. After complete excision with preservation of the capsule, the patient has undergone a dental follow-up with no clinical signs of lesion recurrence and a very satisfactory scar appearance after 7 years.
Keywords: Operative surgical procedures,Parotid neoplasms,Pleomorphic adenoma,Salivary glands.
Resumo
O adenoma pleomórfico é a lesão benigna mais comum das glândulas salivares, afetando principalmente a glândula parótida. A glândula parótida acessória é um tecido salivar separado da glândula parótida e é considerada uma variação anatómica com baixa incidência e raramente afetada por tumores. Uma paciente do sexo feminino, de 20 anos, apresentou queixa de edema com aumento de volume há aproximadamente 18 meses. Ao exame
clínico, foi identificado nódulo móvel localizado na mucosa vestibular, palpável intra e extraoralmente, de consistência firme, assintomático, com contornos bem circunscritos e sem linfadenopatia associada. A ultrassonografia revelou imagem hipoecoica arredondada, sem vascularização associada, na região do ângulo da mandíbula esquerda. Perante essa condição, foi realizada biópsia excisional da lesão sob anestesia local em ambiente ambulatório. No intraoperatório, foi observada lesão nodular encapsulada, cuja localização sugeria origem na glândula parótida acessória. A análise histopatológica confirmou o diagnóstico de adenoma pleomórfico. Após excisão completa com preservação da cápsula, a paciente foi submetida a acompanhamento estomatológico, sem sinais clínicos de recidiva da lesão e com apresentação de cicatriz muito satisfatória após 7 anos.
Palavras-chave: Procedimentos cirúrgicos operatórios, Neoplasias parotídeas, Adenoma pleomórfico, Glândulas salivares.
Introduction
The accessory parotid gland (APG) is considered an anatomical variation that represents a separate tissue of the parotid gland, located anterior to the mandibular branch, between the zygomatic and buccal branches of the facial nerve in the masséter muscle, and closely related to Stensen’s duct.1, 2, 3 Autopsy studies have reported an incidence of 21-69% in human cadavers.1, 4
Lesions arising from the APG are rare, with an incidence of 1% to 8% of all parotid gland tumors.<5 However, when present, these lesions have a higher malignancy rate (26%-55%) than major parotid gland tumors.3, 5 Clinically, APG lesions are de scribed as “soft-tissue masses” located in the middle of the buccal mucosa, usually unilateral, without painful symptoms, slow growing, and sessile due to the fixation to the masseteric fascia.6
Pleomorphic adenoma (PA) is considered the most common salivary gland neoplasm. It manifests in all age groups, with the most frequent involvement in the 30 to 60-year age group and a slight predilection for women.7, 8 PA occurs most commonly in the parotid gland — 40 to 75%, followed by the submandibular gland and minor salivary glands.9, 10 The palate is the most common intraoral site, mainly the hard palate, while occurrences in other intraoral sites include the upper lip and buccal mucosa.11
As in the main parotid gland, PA is the most common benign tumor of the APG. Clinically, it usually presents as a firm, slowly progressive, and painless unilateral swelling, typically without facial nerve involvement.5, 12, 13 However, data on the prevalence of PA in the APG are scarce in the literature. Therefore, the present study aims to elucidate a clinical case of PA in the APG in a young patient.
Case report
A 20-year-old female, systemically healthy, was referred to the stomatology service complaining of a swelling in the right cheek. It had been progressively increasing for approximately 18 months, without painful symptoms, but with aesthetic discomfort.
Ultrasonography revealed a rounded hypoechoic image, without associated vascularization, compatible with a nodule in the angle region of the left mandible (Figure 1). The other structures were preserved, and there was no enlargement of the cervical, submandibular, or parotid lymph nodes. During the extraoral physical examination, a slight swelling was noted just below the zygomatic arch (Figure 2). Intraoral clinical examination revealed the presence of a palpable nodule, both intra- and extraoral, located in the buccal mucosa, which was firm, mobile, asymptomatic, and well-circumscribed. No lymph node enlargement was found in the lateral cervical chains, nor in the submandibular or parotid chains.
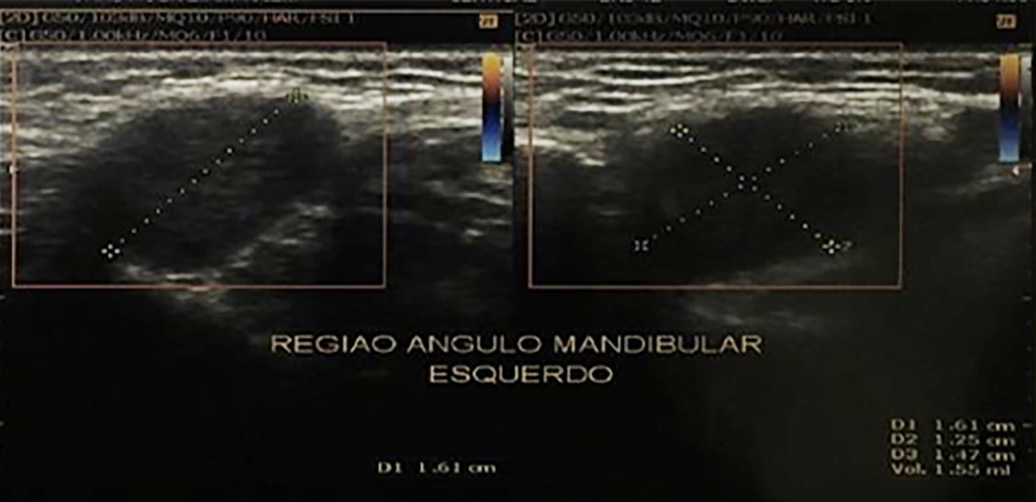
Figure 1. Ultrasonography of the angle region of the left mandible.

Figure 2. Extraoral appearance of the lesion with a slight swelling just below the zygomatic arch.
Based on the diagnostic hypotheses of a dermoid cyst and a sebaceous cyst, enucleation of the mass was performed. The surgical procedure was executed under local infiltrative anestesia with 2% articaine. The intraoperative aspiration biopsy was negative, indicating a solid lesion. An intraoral incision was initiated superiorly to the papilla of the parotid duct. Carefully, continuous blunt dissection (divulsion) was performed meticulously to preserve the surrounding soft tissues (Figure 3A). Intraoperatively, a nodular and encapsulated lesion was observed. This mass was characterized by well-defined borders and was readily separable from the adjacent tissues. The intraoperative
location was highly suggestive of a development arising from the APG. The lesion was entirely removed, ensuring the integrity of the lining capsule was strictly preserved (Figure 3b). Along with the tumor, the entire APG was also excised (Figure 3c). After the complete excision, the buccal fat pad (Bichat’s fat pad) was repositioned to mitigate potential facial asymmetry (Figure 3D). Primary closure was subsequently achieved using a single stitch suture.
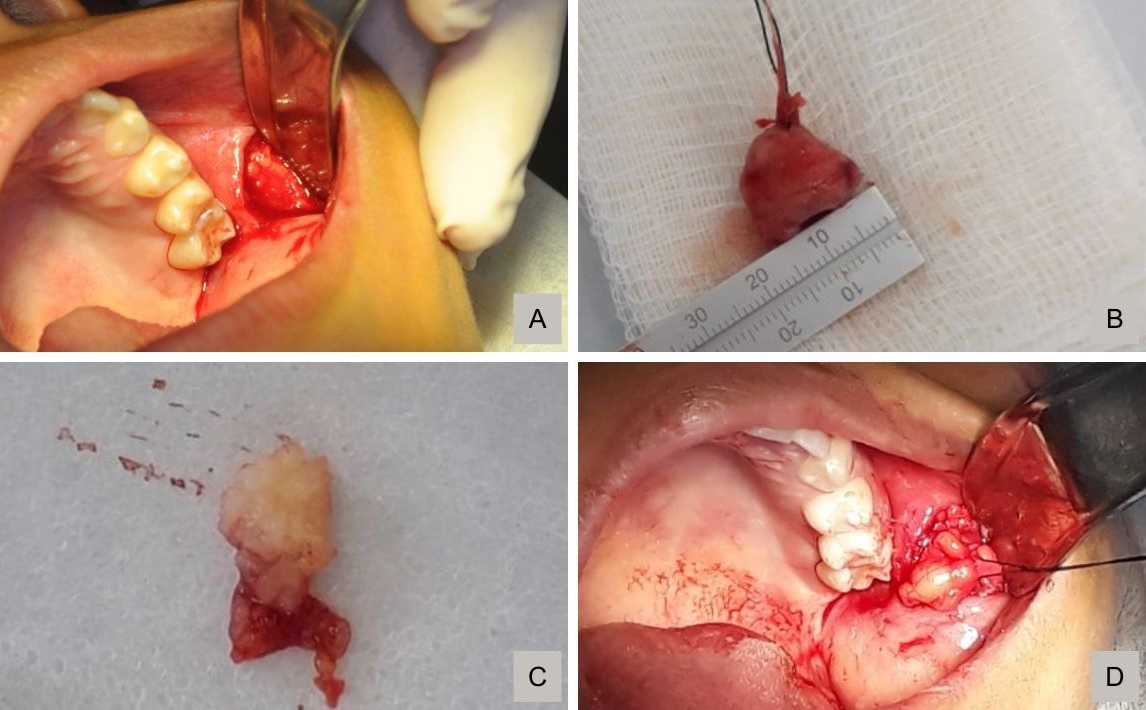
Figure 3. Intraoperative sequence of the transoral excision: A) Identification of a well-defined, encapsulated nodular lesion in the accessory parotid gland region; B) Complete enucleation of the lesion with preservation of the capsule integrity; C) Excision of the entire accessory parotid gland along with the lesion; D) Repositioning of the buccal fat pad (Bichat’s fat pad).
The histopathological analysis showed a benign salivary gland neoplasm with an encapsulated appearance, characterized by the proliferation of epithelial cells forming ductal and cystic spaces, and myoepithelial cells of varying morphology, surrounded by a myxoid stroma and sometimes hyaline (Figure 4). After analysis, a definitive diagnosis of PA was established. After seven year of dental follow-up, the patient has a very satisfactory scar appearance and no clinical signs of lesion recurrence. Informed consent and authorization for the use of the presented clinical data were obtained to ensure the patient’s confidentiality and anonymity, in accordance with applicable ethical guidelines.
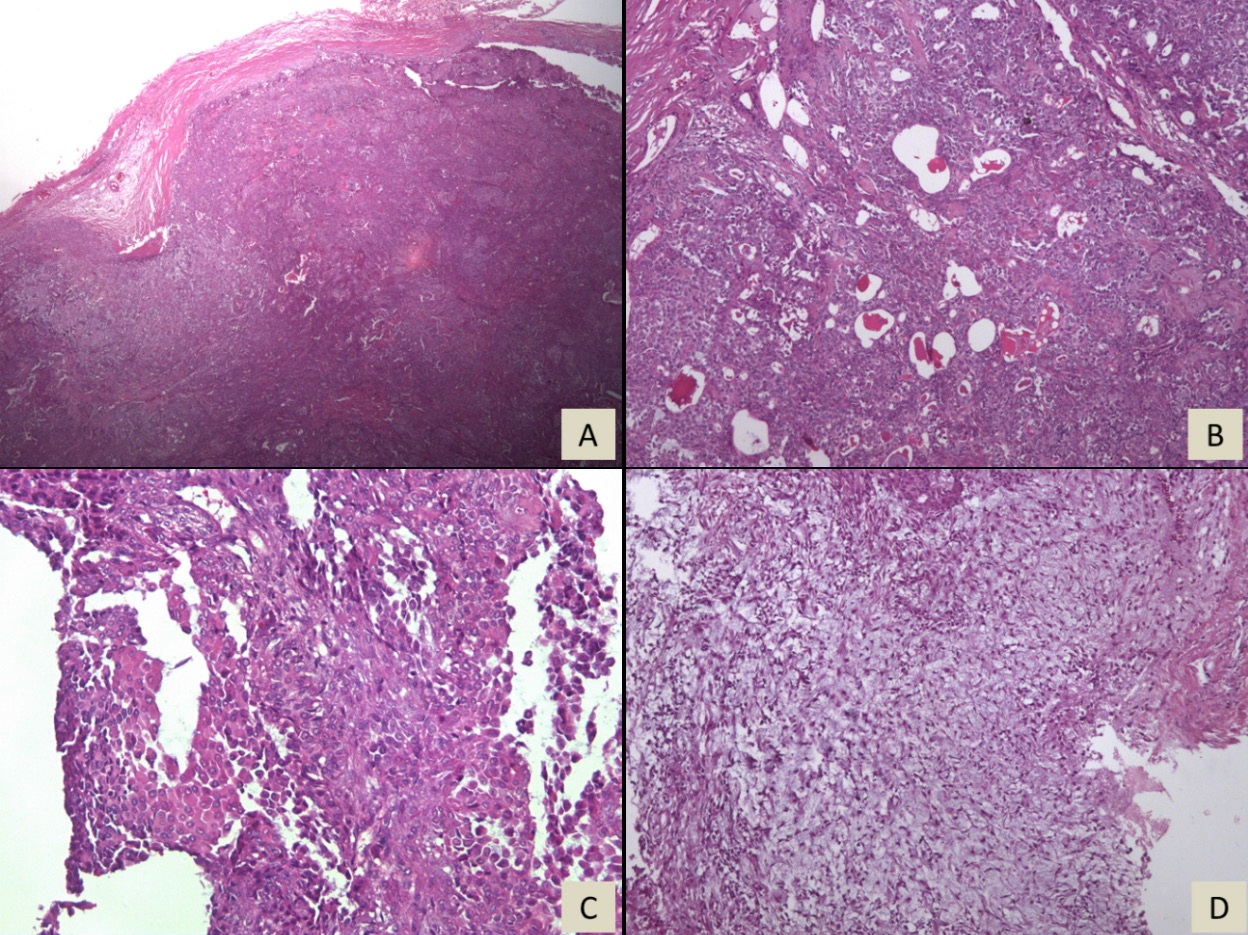
Figure 4. Histopathological examination: A) Neoplasm surrounded by a fibrous capsule; B) Tumor sheet showing ductiform and cystic spaces containing luminal eosinophilic secretion; C) Proliferation of cells with myoepithelial morphology; D) Myxoid stroma.
Discussion and conclusions
PA in the APG is a relatively uncommon condition, scarcelyreported in the literature. Awareness of APG’s existence is the first step in diagnosing pathologies in this structure and, consequently, in choosing the best way to treat tumors satisfactorily and safely, to avoid recurrences and complications.
The APG can serve as a potential site for benign and malignant lesion development, with PA and mucoepidermoid carcinoma as the most common benign and malignant lesions, respectively, in this structure. 6, 14 - 16 However, various lesions may be considered in the differential diagnosis of APG pathologies, including dermoid cyst, schwannoma, lipoma, primary Stensen’s duct tumor, and neurofibroma.17, 18 In the presente case, the diagnostic hypotheses of dermoid cyst and sebaceous cyst were supported by characteristics such as the patient’s age and the lesion’s unusual location. PA in the APG usually presents as a localized, asymptomatic nodule on the right or left buccal mucosa region. The consistency on palpation ranges from firm to rubbery and is often not adherent to the surrounding tissues.17, 18 However, the tumor mass may occasionally be adherent to the tissues.19 Depending on the growth rate of the tumor and its painless nature, the patient may not notice the lesion early, with most cases having a development time of two years or more.6, 17
Imaging tests useful for diagnosing PA in the APG include ultrasonography, magnetic resonance imaging (MRI), and computed tomography (CT); however, CT may not be useful in visualizing the relationship with parotid gland tissue, which is best seen with MRI or CT combined with sialography. Ultrasonography is effective in differentiating cystic from solid masses20 and in identifying soft-tissue tumors.17 In the presente case, ultrasonography was essential to determine the lesion’s location, size, and relationship to anatomical structures, in addition to being useful for surgical planning.
Histologically, the APG is composed of mixed secretor glands with serous and mucous acini, whereas in the parotid gland, only serous acini are present, according to autopsy studies.18, 21 There is controversy in the literature regarding the tumor’s biological behavior, given the difference in cellular composition of the two glands. Some studies report that the highest proportion of malignant tumors occurs in the APG (38.5% to 55%) compared to the parotid gland (25%), while others report no differences in histological findings between PA in the APG and in the main parotid gland.14, 15, 17, 19, 20
In general, certain histopathologic changes may be associated with an increased risk of PA recurrence, such as a stromarich variant with capsular infiltration.21 An increased risk of malignant transformation appears to be associated with focal necrosis, extensive hyalinization, vascular or capsular invasion, hypercellularity, and atypical mitosis.22
The basic treatment for both PA in the APG and other benign neoplasms in the APG consists of a surgical approach.
There is still debate in the literature regarding the ideal technique that combines preservation of anatomical structures with adherence to oncological principles. The main reported approaches are standard parotidectomy, facelift, transcutaneous incisions, and transoral incisions.2 Recurrence rates after surgery or treatment of APG tumors are low, even in cases ofmalignancy, ranging from zero to 9%.22, 23
In the present case, factors such as the patient’s age and the lesion’s early diagnosis, location, and size allowed for a more conservative treatment using the transoral approach, which represents a minimally invasive, anatomically direct technique that provides adequate surgical access without the need for extensive cervicofacial incisions or superficial parotidectomy.
Furthermore, this approach is associated with a lower risk of aesthetic and functional morbidity, including visible scarring and potential facial nerve injury, while offering a favorable risk– benefit profile in the management of APG tumors.24
Although conventional parotidectomy has been reported as the preferred approach for the management of benign lesions in the APG due to its wide exposure and easy access to the lateral lobe,4 the transoral approach offers notable advantages, including shorter operative time, smaller incision, na greater cosmetic satisfaction, with no significant diferences in the incidence of facial nerve paresis or Frey’s syndrome.25
After seven years of follow-up, the patient appears to have had very satisfactory healing and no clinical signs of complications or recurrence.
References
1. Frommer J. The human accessory parotid gland: its incidence, nature, and significance. Oral Surg Oral Med Oral Pathol. 1977;43:671–6.
2. Luksic I, Mamic M, Suton P. Management of accessory parotid gland tumours: 32- year experience from a single institution and review of the literature. Int J Oral Maxillofac Surg. 2019;48:1145–52.
3. Rosa MA, Łazarz DP, Pękala JR, Skinningsrud B, Lauritzen SS, Solewski B, et al. The accessory parotid gland and its clinical significance. J Craniofac Surg. 2020;31:856-60.
4. Pasick LJ, Tong JY, Benito DA, Thakkar P, Goodman JF, Joshi AS. Surgical management and outcomes of accessory parotid gland neoplasms: a systematic review. Am J Otolaryngol. 2020;41:102610.
5. Newberry TR, Kaufmann CR, Miller FR. Review of accessory parotid gland tumors: Pathologic incidence and surgical management. Am J Otolaryngol. 2014;35:48-52.
6. Nemecek JR, Marzek PA, Young VL. Diagnosis and treatment of accessory parotid gland masses. Ann Plast Surg. 1994;33:75–9.
7. Eveson JW, Kusafuka K, Stenman G, Nagao T. Pleomorphic adenoma. In: Barnes L, Eveson JW, Reichart P, Sidransky D editors. World Health Organization Classification of Tumours: Pathology & Genetics – Head and Neck Tumours. Geneva: WHO Press, 2005. p. 254–58. Available from: https://screening.iarc.fr/doc/BB9.pdf.
8. Andreasen S, Therkildsen MH, Bjørndal K, Homøe P. Pleomorphic adenoma of the parotid gland 1985–2010: a Danish nationwide study of incidence, recurrence rate, and malignant transformation. Head Neck. 2016;38(Suppl1):E1364-9.
9. Tian Z, Li L, Wang L, Hu Y, Li J. Salivary gland neoplasms in oral and maxillofacial regions: a 23-year retrospective study of 6982 cases in an eastern Chinese population. Int J Oral Maxillofac Surg. 2010;39:235–42.
10. Fonseca FP, Carvalho MV, de Almeida OP, Rangel ALCA, Takizawa MCH, Bueno AG, et al. Clinicopathologic analysis of 493 cases of salivary gland tumors in a Southern Brazilian population. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:230–9.
11. Nóbrega MQR, Lopes LJ, Cardoso RG, Nonaka CFW, de Souza LB. Minor salivary gland neoplasms: retrospective study of 83 cases. RGO Rev Gaúch Odontol. 2010;58:357–62.
12. Almeslet AS. Pleomorphic adenoma: a systematic review. Int J Clin Pediatr Dent. 2020;13:284-7.
13. Sergi B, Limongelli A, Scarano E, Fetoni AR, Paludetti G. Giant deep lobe parotid gland pleomorphic adenoma involving the parapharyngeal space. Report of three cases and review of the diagnostic and therapeutic approaches. Acta Otorhinolaryngol Ital. 2008;28:261-5.
14. Toh H, Kodama J, Fukuda J, Rittman B, Mackenzie I. Incidence and histology of human accessory parotid glands. Anat Rec.1993;236:586-90
15. Lin DT, Coppit GL, Burkey BB, Netterville JL. Tumors of the Accessory Lobe of the Parotid Gland: A 10-Year Experience. Laryngoscope. 2004;114:1652-5.
16. Koudounarakis E, Karatzanis A, Nikolaou V, Velegrakis G. Pleomorphic adenoma of the accessory parotid gland misdiagnosed as glomus tumour. JRSM Short Rep. 2013;4:23.
17. Lewkowicz A, Levy Y, Zeltser R, Zagury A, Nahlieli O. Accessory parotid gland masses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:610-12.
18. Kakulas EG, Smith AC, Sormann G. Pleomorphic adenoma of the accessory parotid gland. J Oral Maxillofac Surg. 1994;52:867-70.
19. Ramachar SM, Huliyappa HA. Accessory parotid gland tumors. Ann Maxillofac Surg. 2012;2:90-3.
20. Soares AB, Altemani A, de Araújo VC. Study of histopathological, morphological and immunohistochemicalfeatures of recurrent pleomorphic adenoma: an attempt to predict recurrence of pleomorphic adenoma. J Oral Pathol Med. 2011;40(4):352–8.
21. Zbären P, Stauffer E. Pleomorphic adenoma of the parotid gland: histopathologic analysis of the capsular characteristics of 218 tumors. Head Neck. 2007;29:751–7.
22. Jain S, Hasan S, Vyas N, Shah N, Dalal S. Pleomorphic adenoma of the parotid gland: Report of a case with review of literature. Ethiop J Health Sci. 2015;25:189-94.
23. Sun G, Hu Q, Tang E, Yang X, Huang X. Diagnosis and treatment of accessory parotid-gland tumors. J OralMaxillofac Surg. 2009;67:1520–3.
24. Osborne RF. Transoral Parotidectomy. Oral Maxillofac Surg Clin North Am. 2021;33:169-75.
25. Kim JP, Lee DK, Moon JH, Ryu JS, Woo SH. Endoscope-assisted transoral accessory parotid mass excision: multicentre prospective observational study. Laryngoscope. 2020;130:1218-26.
João Vitor Freitas da Silva
E-mail address: onevitor@alu.ufc.br
CRediT authorship contribution statement
Ivana de Sousa Brandão: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. João Vitor Freitas da Silva: Investigation, Visualization, Writing – review & editing. Filipe Nobre Chaves: Methodology, Supervision, Validation. Marcelo Bonifácio da Silva Sampieri: Methodology, Supervision, Validation. Denise Hélen Imaculada Pereira de Oliveira: Methodology, Project administration, Validation, Visualization, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
1646-2890/© 2026 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).