
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2026 | 67 (1) | 34-39
Clinical case
Rapidly growing peripheral giant cell granuloma: A case report
Granuloma periférico de células gigantes de crescimento rápido: Relato de caso
a Faculty of Human Medicine, Antenor Orrego Private University, Trujillo, Peru
b Faculty of Stomatology, National University of Trujillo, Trujillo, Peru
Hector Martin Vargas Cornejo - hmvargasco@unitru.edu.pe
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 67
Issue - 1
Clinical case
Pages - 34-39
Go to Volume
Article History
Received on 24/02/2026
Accepted on 19/04/2026
Available Online on 30/04/2026
Keywords
Clinical Case Report
Rapidly growing peripheral giant cell granuloma: A case report
Granuloma periférico de células gigantes de crescimento rápido: Relato de caso
Edward Henry Miranda Gutiérrez1 0000-0002-2797-138X
Hector Martin Vargas Cornejo2,* 0000-0002-1815-9605
Cesar Augusto Jiménez-Prado2 0000-0002-9444-9188
Manuel Fernando Guillén-Galarza2 0000-0002-9684-9898
1 Faculty of Human Medicine, Antenor Orrego Private University, Trujillo, Peru.
2 Faculty of Stomatology, National University of Trujillo, Trujillo, Peru.
Article history:
Received 24 February 2026
Accepted 19 April 2026
Available online 30 April 2026
Abstract
Peripheral giant cell granuloma is a benign reactive gingival lesion associated with chronic irritation. It typically presents as a reddish-violet mass that tends to bleed or ulcerate and may be associated with underlying bone resorption. A 62-year-old woman presented with a three-month history of a painful, bleeding, pedunculated lesion extending from the right mandibular canine to the second premolar. Radiographic findings suggestive of superficial cortical alteration were observed. The lesion was treated by complete surgical excision using an elliptical incision, including removal of the pedicle and curettage of the underlying periosteum and superficial bone. Histopathological evaluation confirmed the diagnosis of peripheral giant cell granuloma. Local irritative factors were eliminated to reduce the risk of recurrence. At the one-month follow-up, healing was satisfactory. Due to the short follow-up period, recurrence cannot be assessed. This case highlights the importance of early recognition and complete surgical management to prevent bone involvement and guide appropriate treatment.
Keywords: Case reports,Gingival diseases,Giant cell granuloma,Oral pathology.
Resumo
O granuloma periférico de células gigantes é uma lesão gengival reativa benigna associada à irritação crónica. Tipicamente, apresenta-se como uma massa vermelho-violeta com tendência a sangrar ou ulcerar e pode estar associado a reabsorção óssea subjacente. Uma mulher de 62 anos apresentou-se com história de três meses de uma lesão dolorosa, sangrante e pediculada, estendendo-se do canino inferior direito ao segundo pré-molar. Os achados radiográficos sugeriam alteração cortical superficial A lesão foi tratada por excisão cirúrgica completa através de incisão elíptica, incluindo remoção do pedículo e curetagem do periósteo subjacente e do osso superficial. A avaliação histopatológica confirmou o diagnóstico de granuloma periférico de células gigantes. Os fatores irritantes locais foram eliminados para reduzir o risco de recorrência. No acompanhamento de um mês, a cicatrização era satisfatória. Devido ao curto período de acompanhamento, a recorrência não pôde ser avaliada. Este caso destaca a importância do reconhecimento precoce e da abordagem cirúrgica completa para prevenir o envolvimento ósseo e orientar o tratamento adequado.
Palavras-chave: Relatos de Casos,Doenças da Gengiva,Granuloma de Células Gigantes,Patologia Oral.
Introduction
Peripheral giant cell granuloma (PGCG) is a benign reactive lesion that arises from the periosteum or periodontal ligament and develops on the gingiva or alveolar mucosa. Clinically, it appears as an exophytic nodule with a sessile or pedunculated base, usually reddish or purplish in color and with a tendency to bleed.1 – 3 Although it is among the most common reactive gingival lesions, it accounts for only a small proportion of all oral lesions.2, 4 PGCG occurs more often in adult females between the third and sixth decades of life and affects the mandible, especially the anterior region.1, 3 Its occurrence in elderly patients is less common and may pose a diagnostic challenge because of its resemblance to other lesions.3, 4 PGCG usually presents as a slow-growing lesion confined to the gingival soft tissues. However, variations in clinical be havior may occur, and some cases may mimic more aggressive conditions. In particular, rapid enlargement and radiographic signs suggestive of cortical involvement are uncommon features that may complicate the diagnostic approach. Histopathologically, PGCG is characterized by an unencapsulated proliferation of spindle-shaped and polygonal mesenchymal cells, with multinucleated osteoclast-like giant cells embedded in a vascular stroma containing hemosiderin deposits and extravasated red blood cells.1, 4, 5 The differential diagnosis includes pyogenic granuloma, peripheral ossifying fibroma, peripheral odontogenic fibroma, central giant cell granuloma, vascular lesions such as hemangioma, and giant cell lesions associated with systemic conditions, particularly hyperparathyroidism (brown tumor).
These entities may share similar clinical features but differ in histology and biological behavior.4, 5 Histopathologic examination is essential for diagnosis, while radiographic assessment helps rule out bone involvement.2, 4 Treatment consists of surgical excision with curettage of the underlying periosteum or bone and elimination of local irritants to reduce recurrence, which ranges from 2% to 9% depending on the completeness of curettage and control of etiological factors.1, 3, 4
The aim of this report is to describe the clinical course, diagnosis, treatment, and early postoperative follow-up of a patient with PGCG presenting with atypical features. This report was prepared in accordance with the CARE guidelines6 and the corresponding checklist was used during manuscript preparation (Appendix 1). The present case is noteworthy because of the combination of accelerated growth, bleeding tendency, and superficial cortical erosion in an older patient, which raised suspicion for more aggressive or intraosseous lesions. Reporting such presentations helps refine the clinical spectrum of PGCG and highlights the importance of careful clinicoradiographic and histopathological correlation. Therefore, this case is relevant to clinical practice and warrants publication.
Case report
A 62-year-old female homemaker attended the Dentistry Service of the Regional Teaching Hospital of Trujillo for evaluation of an oral swelling that had increased in size for three months. She reported numbness and pain on contact in the right mandibular region. Her medical history was unremarkable; she denied trauma, endocrine disorders, and regular medication use. No relevant psychosocial risk factors were identified.
The lesion had begun approximately three months prior, with a progressive increase in the volume of the mandibular gingiva. Two months before the consultation, the patient began experiencing episodes of bleeding and discomfort on contact.
One month prior, she noted accelerated growth of the lesion accompanied by increased superficial ulceration. On the day of clinical evaluation (day 0), extraoral examination revealed reduced vertical dimension associated with the loss of posterior dental support. There was no facial asymmetry, swelling, or palpable lymphadenopathy. Intraoral examination showed an exophytic, reddish-violet lesion of approximately 20 mm in diameter with a bleeding surface, a relatively fluctuant consistency, and a pedunculated base on the vestibular gingiva extending from tooth 43 to 45 (FDI World Dental Federation notation) (Fig. 1). Although the lesion showed superficial bleeding on manipulation, diascopy (blanching test) was negative, and aspiration using a 25-gauge needle at the lesion base did not yield blood. Clinical palpation indicated a soft tissue lesion without evidence of intraosseous expansion. Periodontal evaluation of the involved teeth (43–45) revealed no deep periodontal pockets or clinical attachment loss suggestive of periodontal bone destruction.

Figure 1. Intraoral view showing a reddish‑violet pedunculated lesion from the permanent mandibular right canine to the permanent mandibular right second premolar (teeth 43–45).
Periodontal probing around teeth 43–45 showed probing depths within normal limits (≤3 mm), without clinical attachment loss. Oral hygiene was poor, with multiple carious lesions. Residual roots were identified in the posterior mandibular region adjacent to the lesion, associated with dental plaque accumulation and calculus deposits. No defective restorations or prosthetic appliances were observed. These findings were considered relevant local irritative factors. The adjacente teeth were preserved, with no significant mobility (grade 0) and no signs of occlusal trauma. Thus, extraction of adjacent teeth was not required.
Panoramic radiography revealed a localized superficial cortical alteration in the region of teeth 43–45, associated with residual roots and extensive carious lesions in both arches.
There was no evidence of a well-defined intraosseous radiolucency or cortical expansion (Fig. 2). Laboratory tests, including complete blood count, coagulation profile, and fasting glucose, were within normal limits.
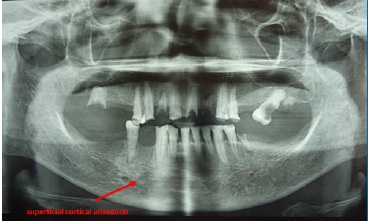
Figure 2. Panoramic radiograph showing superficial cortical alteration in the region of teeth 43–45 and the presence of residual roots and carious lesions.
A differential diagnosis was established based on the observed clinical and radiographic findings: rapid growth, bleeding tendency, radiographic evidence of cortical alteration, negative aspiration findings, and normal periodontal parameters.
Differential diagnoses included pyogenic granuloma, peripheral ossifying fibroma, peripheral odontogenic fibroma, central giant cell granuloma, vascular lesions such as hemangioma, and giant cell lesions associated with systemic conditions, particularly hyperparathyroidism (brown tumor), as summarized in Table 1.
Table 1. Differential diagnosis of a reddish exophytic gingival lesion
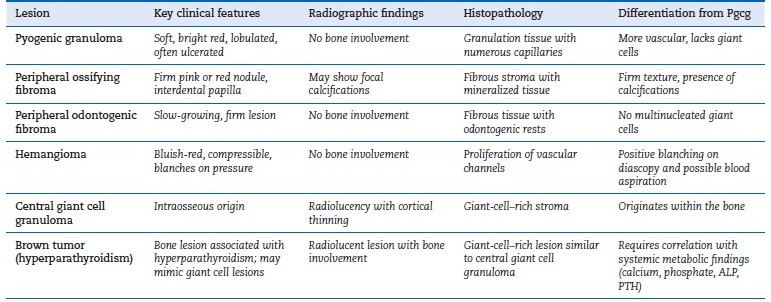
PGCG, peripheral giant cell granuloma.
Three days after the first visit, surgical excision was conducte under local anesthesia with 2% lidocaine and epinephrine (1:100,000), administered by infiltration using one
cartridge (1.8 mL). An elliptical incision was made extending to the periosteum, including a margin of 2–3 mm of clinically healthy surrounding tissue, without flap elevation. The lesion and its pedicle were removed en bloc using a #15 scalpel blade (Fig. 3). Subsequently, thorough curettage of the underlying periosteum and superficial cortical bone was performed using a Lucas-type surgical curette until firm, bleeding bone was reached. Bone margins were then smoothed with a sterile round bur to ensure complete removal of any residual reactive tissue.

Figure 3. Gross view of the excised lesion, showing its pedunculated appearance.
Local irritative factors were carefully identified and managed during the same surgical session, immediately after lesion excision and prior to wound closure. This sequence aimed to prevent contamination of the surgical site and to ensure closure over a field free of chronic irritants. Factors addressed included residual roots and local plaque accumulation in the affected area; the residual roots were extracted, and scaling and root planning of adjacent teeth were performed. No defective restorations or prosthetic factors were identified. Periodontal evaluation revealed no significant tooth mobility or deep periodontal pockets, and all adjacent teeth were preserved.
This comprehensive approach aimed to eliminate potential sources of chronic irritation and reduce the risk of recurrence. Primary closure was achieved using interrupted sutures with non-resorbable silk (3-0). The excised specimen was fixed in 10% neutral buffered formalin and submitted for histopathological examination. Postoperative management included ibuprofen 400 mg every 8 hours for 3 days and 0.12% chlorhexidine mouth rinse twice daily for 7 days; antibiotics were not prescribed. The patient received instructions on oral hygiene and a soft diet during the initial healing period. The total surgical time was approximately 35 minutes. Histopathological analysis confirmed the diagnosis, and surgical margins were reported as free of lesion.
Microscopic analysis showed a non-encapsulated proliferation of connective tissue with a reticular and fibrillar stroma containing numerous multinucleated giant cells and fibroblasts.
The lesion was separated from the overlying stratified squamous epithelium by a band of connective tissue. Foci of hemorrhage and chronic inflammatory infiltrate were presente (Fig. 4). These features were consistent with PGCG.
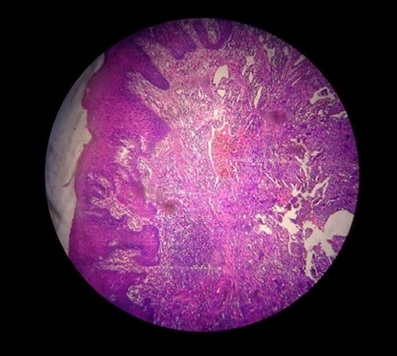
Figure 4. Histopathologic image (H&E, 10×) showing multinucleated giant cells within a fibrovascular stroma.
Postoperative recovery was uneventful. At seven days, the surgical site showed mild erythema and appropriate wound healing.
At the 10-day follow-up, the postoperative course was favorable, with no signs of infection. At 30 days, complete mucosal healing was observed (Fig. 5). The patient reported prompt pain relief, improved oral function, and satisfaction with the outcome.

Figure 5. Postoperative intraoral view at 1-month follow-up showing complete mucosal healing in the region of teeth 43–45, with no clinical signs of early recurrence.
She remains under follow-up. Due to the short follow-up period, long-term outcomes and recurrence risk cannot yet be determined.
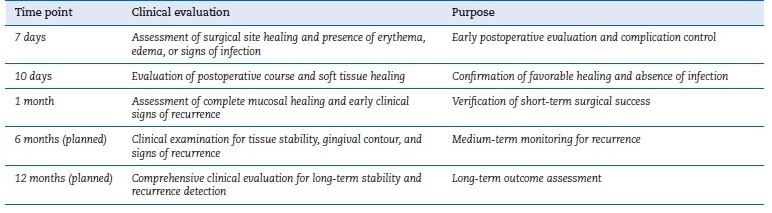
Continued monitoring has been planned according to a structured follow-up schedule (Table 2), including evaluations at 3, 6, and 12 months to assess for possible recurrence.
Table 2. Structured follow-up schedule and clinical objectives
Discussion and conclusions
PGCG is considered a benign reactive lesion triggered by chronic irritation or local trauma rather than a true neoplasm.2, 7 Its etiopathogenesis has been associated with bacterial plaque, calculus, defective restorations, tooth extractions, poorly adapted prostheses, mechanical irritation, and, in some cases, hormonal or metabolic alterations such as hyperparathyroidism.8 These factors are consistent with the clinical context of the present patient, who exhibited poor oral hygiene, residual roots, and multiple local irritants—conditions that likely contributed to lesion development and accelerated growth. PGCG has also been reported in association with dental implants, where chronic irritation, plaque accumulation, or biomechanical factors may contribute to lesion development. Although no implants were present in the current case, this association highlights the broad spectrum of local factors involved in the pathogenesis of PGCG.9
Epidemiologically, PGCG shows a higher prevalence in women between the third and sixth decades of life and affects the mandibular premolar region more often.2, 10, 11 The presente case is consistent with this profile, although the patient’s age (62 years) places her at the upper end of the typical range. This finding reinforces the importance of considering PGCG in older adults, especially when lesions exhibit features that may mimic more aggressive processes.
The lesion size in this case (approximately 20 mm) falls within the range reported in the literature, where PGCG typically measures between 0.5 and 2 cm.7, 12 However, the rapid progression described by the patient is noteworthy. Although PGCG is classically described as slow growing, persistent irritation or repeated trauma may lead to accelerated enlargement.3, 7 This clinical behavior, together with surface bleeding and a reddish- violet appearance, may raise suspicion for more aggressive lesions, highlighting the diagnostic relevance of this case.
Radiographically, PGCG is usually confined to soft tissues; however, superficial bone resorption may occur in long-standing lesions or those associated with persistent chronic irritation.3, 8, 13 In the present case, panoramic imaging demonstrated superficial cortical alteration in the region of teeth 43–45.
While this finding is consistent with existing literature, it is uncommon and may complicate the diagnostic approach. Documenting such presentations is clinically valuable, as evidence of bone involvement may initially raise suspicion for central giant cell granuloma or other intraosseous pathologies. This underscores the importance of correlating radiographic findings with clinical and histopathological features to ensure accurate diagnosis and appropriate management.
The differential diagnosis included pyogenic granuloma, peripheral ossifying fibroma, peripheral odontogenic fibroma, central giant cell granuloma, vascular lesions such as hemangioma, and brown tumor associated with hyperparathyroidism.8, 14 Pyogenic granuloma generally presents with a brighter, lobulated surface and greater vascularity. Peripheral ossifying fibroma typically shows a firm consistency and may contain calcifications or bone formation. Central giant cell granuloma was excluded due to its characteristic radiolucent pattern and because the present case’s findings suggested the bone alteration represented superficial remodeling secondar to a soft tissue lesion, rather than a primary intraosseous process.1, 8 Furthermore, the clinical findings supported superficial vascularization rather than a true vascular lesion, such as hemangioma. In this case, histopathological examination confirmed the diagnosis of PGCG by demonstrating multinucleated giant cells within a fibrovascular stroma, accompanied by hemorrhage and inflammatory infiltrate, in accordance with classical descriptions.15, 16
Total excision with curettage of the underlying periosteum or bone remains the treatment of choice and is essential to reduce recurrence, which has been reported between 2% and 9%.10, 17 A large review including 2,824 cases reported an overall recurrence rate of approximately 9.5% after treatment, reinforcing the importance of complete excision and elimination of local irritative factors.18 In this case, clinical findings at one month indicated satisfactory postoperative healing. However, as recurrence may occur several months after treatment, this short follow-up period does not allow assessment of long-term stability, and continued monitoring is required. Proper management of predisposing factors is also critical, as incomplete excision or persistent local irritation are important contributors to lesion regrowth.13, 18
This report has several limitations. First, the follow-up period is limited to one month, and no additional follow-up data are currently available. Therefore, long-term outcomes and recurrence risk cannot be assessed, representing an important limitation.
Second, no comprehensive metabolic screening was performed to rule out systemic conditions associated with giant cell lesions, such as hyperparathyroidism (brown tumor); only basic laboratory tests were obtained. Although no clinical signs of endocrine disorders were present and the laboratory results were within normal limits, the absence of additional metabolic tests (serum calcium, phosphate, alkaline phosphatase, and parathyroid hormone) represents a limitation. Third, advanced imaging studies, such as periapical radiographs or cone-beam computed tomography, were not performed; therefore, assessment of cortical bone involvement relied solely on panoramicradiography, which has inherent limitations and may not accurately differentiate between superficial cortical alteration, pressure remodeling, or projection artifacts. Finally, as a single case report, these findings cannot be generalized, although they contribute to expanding the clinical spectrum of PGCG. No financial, cultural, or language barriers were encountered during the diagnostic process.
In conclusion, this uncommon presentation of PGCG in na older adult mimicked a more aggressive lesion, underscoring the importance of comprehensive clinical, radiographic, and histopathological correlation to avoid overtreatment. This case highlights relevant diagnostic challenges and provides educational value for the management of reactive gingival lesions, supporting its relevance in clinical practice and justifying its publication. Complete excision with removal of local irritants resulted in satisfactory short-term healing. However, the limited follow-up does not allow assessment of recurrence, and long-term monitoring remains essential.
References
1. Cahuana P, Brunet L, Suñol M, Miranda J. Expansive oral giant cell granuloma in a pediatric patient. Int J Clin Pediatr Dent. 2023;16:405-8.
2. Yousefian M, Aghakouchakzadeh A, Torki S. Peripheral giant cell granuloma as a sign of hyperparathyroidism in a patient under hemodialysis: A case report and review of literature. Clin Case Rep. 2023;11:e7823.
3. Sharma M, Sarma MK, Choudhury D, Rao S, Santosh B, Debnath A, et al. Peripheral giant cell granuloma: A case report of a 9-year-old male child. J Pharm Bioallied Sci. 2024;16(Suppl 3):S2968-71.
4. Sllamniku Z, Krasniqi MS, Kondirolli L. Excision of a benign peripheral giant cell granuloma in the oral mucosa of the anterior mandibular teeth with a 975-nm diode laser: A case report of a 39-year-old woman. Am J Case Rep. 2023;24:e938793.
5. Akerzoul N, Touré B. Surgical excision of peripheral giant cell granuloma of the maxilla: A case report. Pan Afr Med J. 2023;44:141.
6. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE guidelines: Consensus-based clinical case reporting guideline development. Headache. 2013;53:1541-7.
7. Patil CL, Gaikwad RP, Banodkar AB, Attar NB, Sethna GD. Peripheral giant cell granuloma manifestation in pregnancy. Indian J Dent Res. 2018;29:678-82.
8. Limongelli L, Tempesta A, Lauritano D, Maiorano E, Ingravallo G, Favia G, et al. Peripheral giant cell granuloma of the jaws as first sign of primary hyperparathyroidism: a case series. J Clin Med. 2020;9:4042.
9. Mirebeigi SS, Atarbashi MF, Atarbashi MS. Oral lesions associated with dental implants: A retrospective study. BMC Oral Health. 2025;25:1486.
10. Fligelstone S, Ashworth D. Peripheral giant cell granuloma: A case series and brief review. Ann R Coll Surg Engl. 2024;106:649-51.
11. Chicllasto N, Alonso C, Ballón Y. Granuloma periférico de células gigantes atípico: Un dilema diagnóstico. Ver Antoniana Estomatol. 2025;1:138-40.
12. Dodal KA, Vishnani R, Reche A, Bhowate RR, Rajanikanth K. A case study on pyogenic granuloma with review of the literature: An unexpected sequela or a complication of dental extraction? Cureus. 2023;15:e46592.
13. Wu YH, Wu YC, Lee YP, Chiang CP. Peripheral giant cell granuloma: Case report. J Dent Sci. 2022;17:1434-6.
14. Rodrigues SV, Mitra DK, Pawar SD, Vijayakar HN. Peripheral giant cell granuloma: This enormity is a rarity. J Indian Soc Periodontol. 2015;19:466-9.
15. Gao X, Wang S, Zhan X, Liu Y, Chen L, Sun J, et al. Giant cell lesions in the maxillofacial region: Diagnostic points and treatment strategies. Front Oncol. 2025;15:1572560.
16. Sahoo NK, Mowar A, Dubey P, Maheshwari I. An audit of histopathological pattern of peripheral giant cell granuloma: A retrospective study. Ann Maxillofac Surg. 2024;14:62-5.
17. Chrcanovic BR, Gomes CC, Gomez RS. Peripheral giant cell granuloma associated with dental implants: A systematic review. J Stomatol Oral Maxillofac Surg. 2019;120:456-61.
18. Brar GK, Sodhi SPS, Malhotra M, Goyal P. A rare case of peripheral giant cell granuloma. Int J Oral Health Dent. 2021;7:138-41.
Hector Martin Vargas Cornejo
E-mail address: hmvargasco@unitru.edu.pe
CRediT authorship contribution statement
Edward Henry Miranda Gutiérrez: Conceptualization, Data curation, Formal analysis, Methodology, Investigation, Writing – original draft. Hector Martin Vargas Cornejo: Writing – review & editing. Cesar Augusto Jiménez-Prado: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. Manuel Fernando Guillén-Galarza: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Appendices. Supplementary content
Supplementary data associated with this article can be found, in
the online version, at https://administracao.spemd.pt/app/assets/imagens/files_img/1_19_6a16a58d87e74.pdf
1646-2890/© 2026 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).