
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2026 | 67 (1) | 11-20
Original research
Oral health-related attitudes and behaviors in Portuguese Air Force military personnel
Atitudes e comportamentos relacionados com a saúde oral de militares da Força Aérea Portuguesa
a Portuguese Air Force, Lisbon, Portugal
b Universidade de Lisboa, Faculdade de Medicina Dentária, Lisbon, Portugal
c Unidade de Investigação e Ciências Orais e Biomédicas (UICOB), Faculdade de Medicina Dentária, Universidade de Lisboa, Lisbon, Portugal
Sónia Ferreira - soniaferreira@campus.ul.pt
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 67
Issue - 1
Original research
Pages - 11-20
Go to Volume
Article History
Received on 31/07/2025
Accepted on 21/04/2026
Available Online on 30/04/2026
Keywords
Original Research
Oral health-related attitudes and behaviors in Portuguese Air Force military personnel
Atitudes e comportamentos relacionados com a saúde oral de militares da Força Aérea Portuguesa
Sónia Ferreira1,2,* 0000-0002-5292-1544
Sónia Mendes2,3 0000-0001-8831-5872
Mário Bernardo2,3 0000-0002-9204-7230
1 Portuguese Air Force, Lisbon, Portugal
2 Universidade de Lisboa, Faculdade de Medicina Dentária, Lisbon, Portugal
3 Unidade de Investigação e Ciências Orais e Biomédicas (UICOB), Faculdade de Medicina Dentária, Universidade de Lisboa, Lisbon, Portugal
Article history:
Received 31 July 2025
Accepted 21 April 2026
Available online 30 April 2026
Abstract
Objectives: The Armed Forces require ready and healthy military personnel with good oral health to avoid medical and dental emergencies. This study aimed to investigate oral health-related behaviors and attitudes among Portuguese Air Force personnel and identify areas for improvement.
Methods: A cross-sectional study was conducted on active-duty military personnel from the Portuguese Air Force. Participants voluntarily completed the study questionnaire sent via email. The questionnaire gathered information on demographics, attitudes and behaviors related to oral health, as well as self-reported oral health issues. The study of attitudes and behaviors included the Portuguese version of the HUDBI (Hiroshima University Dental Behavioral Inventory). Statistical analyses used Mann-Whitney and Kruskal-Wallis tests (α=0.05).
Results: The sample included 360 participants, representing 11.2% of the entire target population. The mean HUDBI score was 6.82 (SD=1.61). Most military personnel reported brushing their teeth at least twice a day with fluoride toothpaste. Only 12.8% reported using dental floss on a daily basis. There was a significant association between HUDBI and age group (p=0.045), military position (p=0.026), level of education (p=0.039), flossing (p<0.001), and toothbrushing frequency (p=0.004).
Conclusions: HUDBI values were reasonable, and twice-daily toothbrushing was widely adopted, but daily flossing was infrequent. Oral health attitudes and behaviors were better among older individuals, those with higher military positions, a higher level of education, and those who brushed and flossed more frequently. These relationships should be considered for improving the oral health of the population.
Keywords: Attitude to health, Health behavior, Military personnel, Mouth diseases, Oral health.
Resumo
Objetivos: As Forças Armadas necessitam de militares prontos e saudáveis, com boa saúde oral, a fim de evitar emergências médicas. Este estudo pretendeu investigar comportamentos e atitudes relacionados com a saúde oral entre os militares da Força Aérea Portuguesa e identificar áreas de melhoria.
Métodos: Foi realizado um estudo transversal com militares no ativo da Força Aérea Portuguesa. Os participantes preencheram voluntariamente o questionário enviado por e-mail, sendo recolhidas informações demográficas, atitudes e comportamentos de saúde oral, bem como problemas de saúde oral autorrelatados. Também foi incluída no questionário a versão portuguesa do HUDBI (Hiroshima University Dental Behavioral Inventory). A análise
estatística utilizou os testes de Mann-Whitney e Kruskal-Wallis (α=0,05).
Resultados: A amostra incluiu 360 participantes (11,8% da população-alvo). O valor médio do HUDBI foi 6,82 (dp=1,61). A maioria dos militares escovava os dentes pelo menos bidiariamente com dentífrico fluoretado. Apenas 12,8% referiu usar fio dentário diariamente. Houve associação entre o HUDBI e a faixa etária (p=0,045), a posição militar (p=0,026), o nível de escolaridade (p=0,039), o uso do fio dentário (p<0,001) e a frequência de escovagem (p=0,004).
Conclusões: Os valores de HUDBI foram razoáveis e a escovagem dentária bidiária verificou-se bem implementada. No entanto, o uso diário do fio dentário foi pouco frequente. As atitudes e comportamentos foram melhores nos indivíduos mais velhos, com posições militares mais elevadas, nível de escolaridade mais elevado e que escovavam e usavam fio dentário com maior frequência. Estas relações devem ser consideradas para a melhoria da saúde oral da população.
Palavras-chave: Atitudes para a Saúde,Comportamentos de Saúde,Militares,Doenças da Boca,Saúde Oral.
Introduction
Oral health is an essential part of overall health, acting as a significant determinant of an individual’s quality of life and sharing several risk factors with other aspects of general health.1 Several oral pathologies are associated with chronic diseases, with examples including poor oral health and diabetes mellitus2 or chronic obstructive pulmonary disease.3
Therefore, oral disease prevention is important not only for maintaining good oral health but also for supporting overall well-being.
The Armed Forces require individuals who are military-ready, fit, healthy, and mobile.4 Good oral health is particularly important, as the opposite can lead to emergencies during service or missions.5 Dental emergencies can disrupt operations and may even require medical evacuation6, ultimately undermining the unit’s overall effectiveness and the success of the mission.7
Within the Armed Forces, aviation plays a key role by increasing the mobility of ground forces. Due to variations in temperature, pressure, and ergonomic factors, aviation activities consistently expose personnel to the physiological effects of physical and mechanical hazards, which can negatively impact the stomatognathic system.8 Furthermore, mission deployment represents a stressful period with challenging living conditions, requiring a high-calorie diet because of the physical exertion involved and the mission’s intensity. During missions, unhealthy behaviors such as smoking and oral hygiene negligence may become more common.9 All these factos can cause underlying asymptomatic oral conditions to manifest symptoms,10leading to emergencies that could be avoided. Therefore, studying the factors that influence the oral health of Armed Forces personnel is essential for preventing oral diseases and their various consequences.
A recent study on Air Force cadets revealed that, despite their young age and military fitness, nearly half showed clinical signs of periodontal disease.11 Another study conducted in 2018 with data from an army regiment in Viseu reported high dental caries prevalence (51.6%) and high plaque index values in 58.2% of military personnel.12 These previous studies reveal indicators of poor oral health, highlighting the need for intervention and preventive measures. Research on oral health among the Portuguese military population remains limited, and collecting current data, particularly across all ages and military ranks, is necessary to develop more effective prevention strategies and promote oral health.
Attitudes and behaviors play a decisive role in oral health, as they directly influence preventive practices and adherence to oral hygiene and dental care.13 The Hiroshima University Dental Behavioral Inventory (HUDBI), developed by Kawamura,14 is one of the instruments available in the literature for assessing the attitudes and oral health behaviors of adults. This instrument has already been validated for the Portuguese population15 and has been used in several Portuguese studies.16 - 20
This study aims to explore oral health-related attitudes and behaviors among active-duty personnel of the Portuguese Air Force, identify their self-reported oral health problems, and analyze the relationship between self-reported oral health problems and oral health attitudes and behaviors.
Material and methods
This cross-sectional study was reviewed and approved by the Portuguese Air Force’s Ethics Committee for Health and Directorate of Health (ref no. 01/2020).
The study population consisted of Portuguese Air Force military personnel on active duty in 2021. All individuals who voluntarily completed the questionnaire and attended an oral health appointment that year were included in the study. The questionnaire was created on an online platform and made accessible to potential participants via an email link. The email message and the first page of the questionnaire included a
brief explanation of the study’s objectives and procedures, concluding with a mandatory question regarding informed and voluntary participation.
Air Force services (Directorate of Communications and Information Systems and Public Relations) distributed the questionnaire electronically to potential participants in February 2021, and sent two subsequent follow-up emails between March and May of the same year to optimize response rates.
The questionnaire was also made available on the Portuguese Air Force Internal Portal.
The questionnaire was specifically designed for this study, based on a literature review.14, 15, 19, 20 Before its final implementation, it was reviewed by two experts experienced in questionnaire research and pre-tested with three individuals to assess the clarity of the questions. After explaining the objectives and procedures of th study, the questionnaire included an initial section to verify inclusion criteria and obtain informed consent. Participants who met the criteria then proceeded to the main questionnaire, which gathered information on demographic details, oral health-related attitudes and behaviors, and self-reported oral health status. The section on behaviors and attitudes incorporated the Portuguese version of the HUDBI.15
The HUDBI comprises 21 dichotomous response items for participants to indicate whether they agree or disagree with each item. Its total score is calculated by summing the scores of 12 of the 21 items, with a maximum of 12 points. Lower scores reflect less positive oral health-related attitudes and behaviors. The total HUDBI score for each individual was calculated by adding 1 point for each correct response to one of the 12 items included in this total: items 2, 4, 6, 8, 9, 10, 11, 12,14, 15, 16, 19.14
Statistical analysis was conducted using SPSS, including descriptive analyses of all variables. For numerical variables, the mean, median, and standard deviation were also calculated.
The relationships between variables were examined using the Mann-Whitney U and Kruskal-Wallis tests at the 0.05 significance level.
Results
Out of a total of 3217 military personnel, 437 responses were collected. After applying the inclusion and exclusion criteria, the final sample comprised 360 individuals, representing 11.2% of the entire target population. Participants from all deployment units were included in the study, with the largest groups being from the Air Force General Staff (21.4%), Air Base 1 (10.8%), Air Base 6 (12.2%), and the Lisbon Pole of the Armed Forces Hospital (8.3%).
The mean HUDBI score was 6.82 (SD=1.61), with a median of 7 (range: 1–10). The items with the highest percentage of agreement were concerns about bad breath (96.1%), tooth color (95.0%), and gum color (75.3%) (Table 1).
Table 1. Frequency of the HUDBI items (n=360).
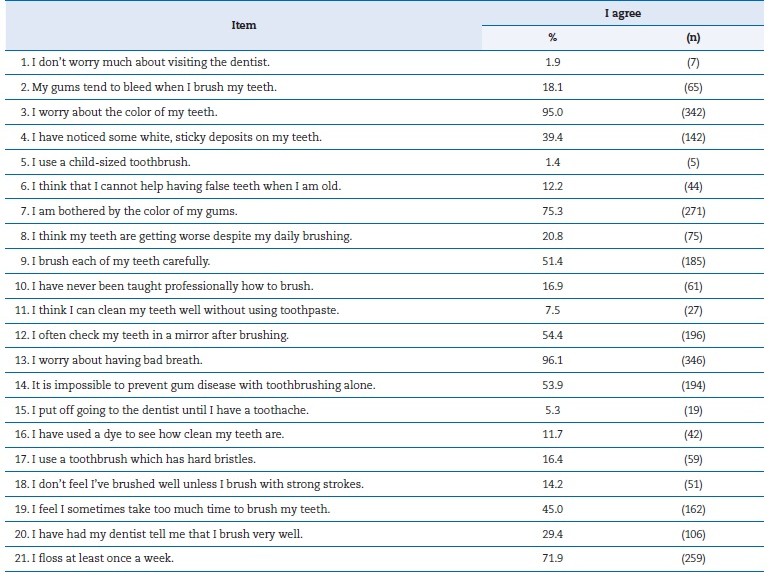
Table 2 displays the sample’s sociodemographic and military characteristics, along with their relationship to the respective HUDBI scores. Most military participants were male (83.9%), and the most common age group was 40-49 years old (32.6%). The military rank with the highest representation was Sergeant (66.1%), and most participants reported having completed secondary education (12 years of schooling) (63.9%).
Table 2. Sociodemographic and military characteristics of the sample and their relationship with HUDBI (n=360).
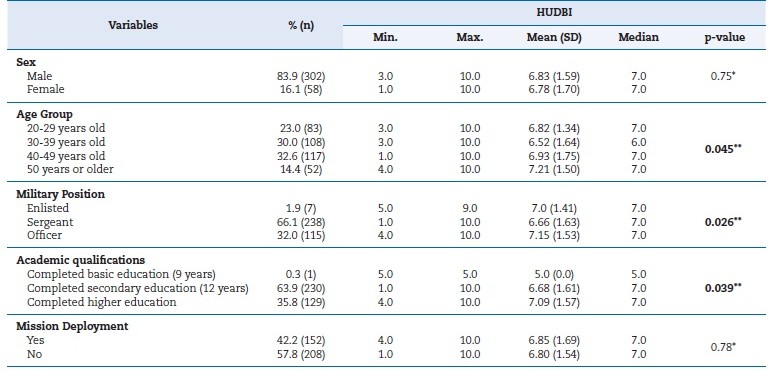
The p-values in bold indicate statistically significant differences.
*Mann-Whitney test. **Kruskal-Wallis test.
A statistically significant relationship was found between HUDBI scores and the age group (p=0.045), military position (p=0.026), and education level (p=0.039). Higher HUDBI scores, indicating better behaviors and attitudes, were observed in the 50+ age group, among officers, and in participants with a completed university degree (Table 2).
Regarding oral health behaviors, most participants cited routine procedures as the reason for visiting the dentist in the past year, specifically “cleaning” (30.3%) or preventive visits (28.3%) (Figure 1). Most military personnel reported brushing their teeth at least twice daily (81.9%) with fluoride toothpaste (88.6%). Only 12.8% reported flossing daily (Table 3). The most common time for brushing was “before going to bed” (81.1%) (Figure 2). A significant association was found between the HUDBI and the frequency of brushing (p=0.004) and flossin (p<0.001), with military personnel who brush and floss more frequently having higher HUDBI scores. The vast majority (91.7%) reported having received information about oral health care from an oral health professional. Moreover, most participants (70.3%) reported “occasional” consumption of sugary foods (Table 3).
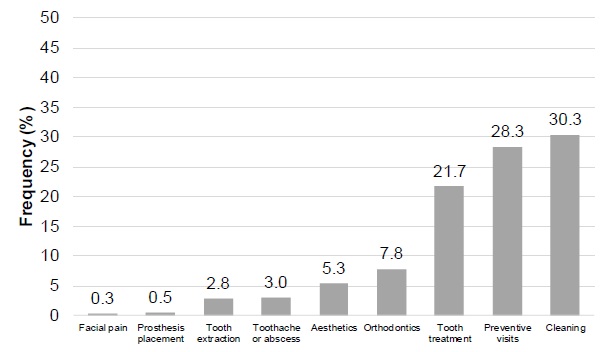
Figure 1. Reason for the last oral health appointment (n=360).
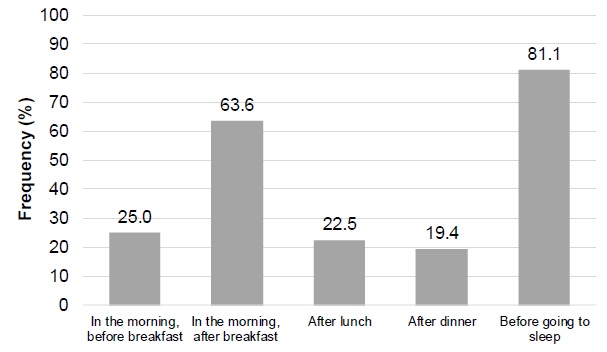
Figure 2. Brushing time (n=360).
Table 3. Oral health-related behaviors and relationship to HUDBI (n=360).
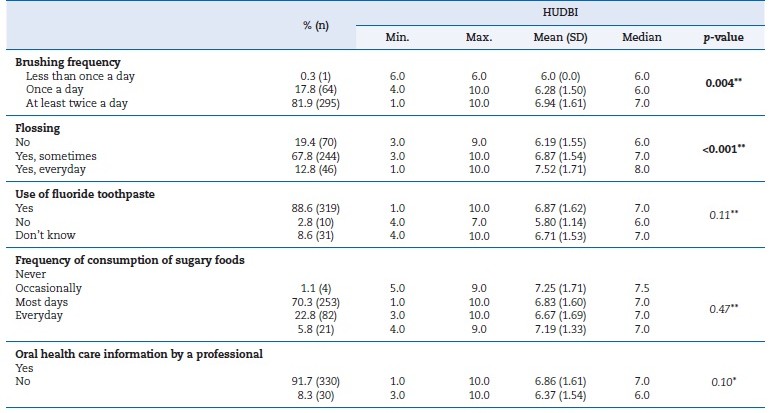
The p-values in bold indicate statistically significant differences.
*Mann-Whitney test. **Kruskal-Wallis test.
The most common self-reported oral health problems among the military were recurrent aphthous stomatitis (51.9%), tooth decay (46.1%), and tooth sensitivity (36.7%) (Figure 3). Only 6.1% of participants reported no oral health problems in the past year. Nearly all respondents (99.1%) reported having more than 20 natural teeth. A significant association was found between HUDBI score and gingival bleeding (p<0.001), canker sores (p=0.002), and dental trauma (p<0.001). Military personnel who reported gingival bleeding or recurrent aphthous stomatitis had lower HUDBI scores. Conversely, those who reported dental trauma showed higher index values (Table 4).
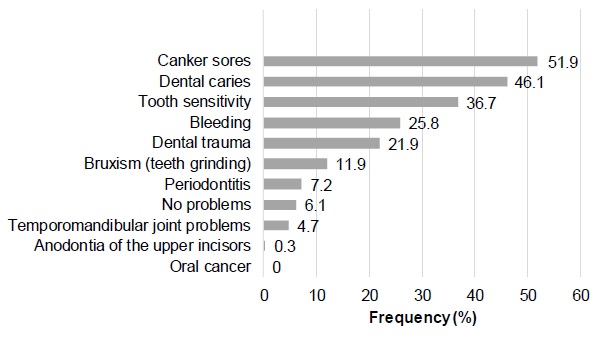
Figure 3. Self-reported oral health problems (n=360).
Table 4. Self-reported health status and oral health status and relationship to HUDBI (n=360).
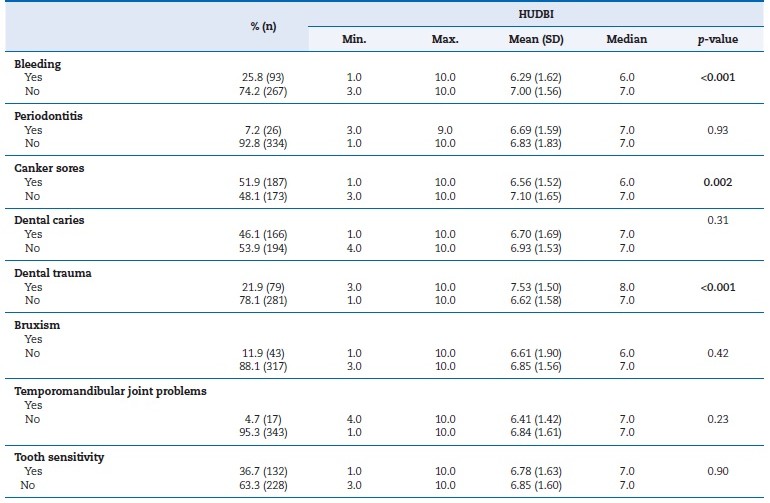
The p-values in bold indicate statistically significant differences. Mann-Whitney test.
Discussion
Military personnel require full physical and mental health due to the physical demands, responsibility, and stress associated with daily military tasks.21 Therefore, it is important to study oral health-related knowledge, attitudes, and behaviors among military personnel, considering the consequences that neglect may cause in daily military life. Additionally, good oral health is vital not only for immediate deployment but also for the
well-being necessary to carry out missions effectively.22, 23 As a result, identifying oral health behaviors that need improvement is essential for the development of strategies to enhance the oral health of military personnel.
The mean HUDBI score in this study was 6.82, reflecting a reasonable overall level of oral health-related knowledge and attitudes but also indicating potential for further improvement. This score was higher than those reported for Israeli army recruits (5.8)24 and Paraguayan Air Force recruits (6.33).25
Conversely, it was slightly lower than the score reported in a Portuguese non-military population of students studying oral health (7.3)19 Despite opportunities for improvement in both samples from Portugal, the similarity between these scores suggests that the military participants in the current study demonstrated notably positive results, highlighting relatively good oral health-related knowledge and attitudes among militar personnel compared to a Portuguese civilian population specialized in oral health.
The HUDBI items that reflected more positive behaviors and attitudes indicated concerns about bad breath, tooth color, gum color, and dental visits. This pattern is consistent with findings reported among Paraguayan recruits, in whom concerns about tooth color (92%) and bad breath (96%) were among the most positively endorsed HUDBI items.25 In other populations, the same items included careful brushing of teeth, checking teeth after brushing, and concerns about bad breath.26 Therefore, the population in this study shows a greater concern with items related to the aesthetic and social aspects of oral health, which oral health professionals can use to motivate military personnel to adopt healthier oral health behaviors.
Regarding less positive oral health-related attitudes and beliefs, a large percentage of the military sample (53.9%) believed that it was impossible to prevent gum disease through toothbrushing alone (item 14). Also noteworthy is the lack of awareness among this population of the presence of bacterial plaque on their teeth (item 4). Similar limited awareness of dental plaque has been reported among Paraguayan recruits, with nearly half failing to recognize plaque accumulation.25 These less-rated items could also be included in oral health appointments to improve behaviors and attitudes. For example, the oral health professional should guide all their patients on how to brush their teeth, using plaque dye to visually demonstrate areas where brushing is ineffective.
They should also explain and demonstrate how to brush carefully and check whether the teeth have been brushed properly. It is important to clarify that brushing takes only about 2 minutes and is a key step in maintaining healthy teeth and gums.
The most favorable oral health-related behaviors and attitudes were observed among military personnel aged 50 years or older, holding officer ranks, and possessing higher levels of education. Evidence from civilian populations suggests a correlation between advanced education and higher health literacy.27, 28 Given that officer rank is typically contingent on higher academic qualifications, these findings suggest that oral health professionals should target interventions for military members with lower educational attainment and lower ranks to reduce oral health disparities within the population.
Most participants reported that “cleaning” and preventive visits were the reasons for their most recent dental visit. Percentages were slightly higher than those found in the general Portuguese population (58.6% versus 56%, respectively).29
Access to oral health care within the military environment is facilitated by the requirement for mandatory annual dental appointments for all active military personnel and by the emphasis on dental fitness necessary for participation in missions, often scheduled at short notice. During these appointments, in addition to assessing oral health status and treatment needs, education and motivation on oral health self-care are also provided. In contrast, the Paraguayan recruits reported difficulties accessing dental services due to conflicts between appointment schedules and intensive training routines, which may compromise both preventive care and oral hygiene guidance.25 Within the Portuguese Air Force, however, structured preventive policies and systematic dental follow-ups appear to support greater adherence to recommended oral health behaviors. Differences in institutional context and access to preventive care may therefore partly explain the more favorable behavioral profiles observed in this study population.
In the present study, 81.9% of the military brushed their teeth at least twice a day, higher than the Portuguese Air Force cadets (63.3%),11 the Dutch army (69%),30 the Croatian army (60%),31 and the general Portuguese population (74.4%).29
Conversely, only 12.8% of participants flossed daily, a figure similar to that of the Dutch army (13%),30 but less frequente than that of Paraguayan recruits (22%)25 and the general Portuguese population (26.3%).29 Other studies of the Portuguese Army12 and Navy32 reported higher rates of daily flossing, at 18% and 42.8%, respectively. These findings indicate that suboptimal flossing remains a significant challenge across diverse civil and military adult populations. On the other hand, data on sugary food consumption are quite limited and infrequente compared to other military populations, such as the US Air Force,33 the Iranian Armed Forces,34 and the Serbian military.35
A positive and statistically significant relationship was observed between the frequency of brushing and flossing and HUDBI scores. This positive relationship was also identified in other populations,< 17 - 20 emphasizing the importance of oral health self-care and its promotion by oral health professionals.
Most participants (91.7%) received information from a health professional on how to care for their teeth and gums during dental appointments. Among Paraguayan recruits, a large majority (87%) stated that they had been professionally instructed on toothbrushing techniques.25 The result of this study is notably higher than that of other military populations, such as the Iranian Air Force (27.8%).33> These findings may be attributed to the well-established preventive oral health policy in the Portuguese Air Force, as well as the easy access to nutrition appointments at the Armed Forces Hospital.
However, despite the mandatory annual appointment in the Portuguese Air Force, the high self-reported prevalence of dental caries underscores the need to strengthen preventive measures during this visit to improve military personnel’s oral health. Soldiers with poor oral health may be unavailable for duty until they complete their dental treatment, affecting their readiness.
There was a statistically significant association between HUDBI scores and gingival bleeding and canker sores. The military personnel who reported these oral problems had lower mean HUDBI scores. Poor oral hygiene, dental problems, or an unbalanced diet are considered risk factors for canker sores.36 In turn, gingival bleeding can be caused by bacterial plaque and by hormonal, nutritional, and medication-related factors.36 To address these oral health problems, effective plaque control through proper oral hygiene self-care is essential.
It was also found that higher HUDBI scores were associated with a higher prevalence of dental trauma. This is an accidental oral health problem and is not dependent on specific oral health behaviors adopted, so the observed association is likely due to a confounding factor. Nevertheless, during military service and participation in military physical training, individuals are more likely to experience dental trauma thanin civilian life,38 which emphasizes the importance of promoting mouthguard use during risky activities.
This study has a few limitations to consider. Being a cross-sectional study, causal relationships cannot be ascertained. Since the sample used in this study is non-probabilistic and accounts for only 11.2% of the target population, caution is required when extrapolating the results. Despite this, according to data from the Portuguese Air Force Data Department, the distributions of military category, level of education, and gender in this study correspond to those in the Portuguese Air Force military population, indicating a sample with a good distribution of these characteristics. Another limitation of this study is the reliance on self-reported oral health problems, which, in addition to being subjective, might overlook subclinical conditions not perceived by participants.
Additionally, the statistical analysis tests used are bivariate, assessing only the relationship between two variables at a time and not controlling for the effects of other potentially relevant variables. Finally, the study focused on military personnel who had attended their mandatory anual appointments. Future studies should compare those who attended with those who did not, to assess potential diferences in oral health outcomes. Even considering these limitations, the present study provides valuable information for an under-researched population and can inform the planning of additional studies and the implementation of targeted oral health promotion strategies.
Conclusions
The HUDBI scores of the study population are reasonable but have potential for improvement. Twice-daily brushing was widely adopted, whereas dental floss was less common. Oral health attitudes and behaviors were better among older individuals, those with higher military ranks, those with higher levels of education, and those who brushed and flossed more frequently. A significant proportion of the military population reported having caries and dental trauma, emphasizing the need to reinforce preventive strategies and oral health education programs.
References
1. FDI World Dental Federation. FDI policy statement on oral health and quality of life. Int Dent J. 2020;66:11–2.
2. Monteiro R. Qualidade de vida relacionada com a saúde oral em pacientes com diabetes tipo 2: relação com variáveis sociodemográficas, comportamentais e clínicas [tese]. Lisboa: Universidade Nova de Lisboa – Escola Nacional de Saúde Pública; 2018.
3. Lago CCL, Camelier FWR, Santos CO, Coutinho MR, Bittencourt S, Camelier AA. Associação entre a doença periodontal e a doença pulmonar obstrutiva crônica: uma revisão de literatura. J Dent Public Health. 2018;9:121–34.
4. Ferrão A, Sousa I. Padrões de aptidão dentária para o pessoal navegante militar em missões OTAN. Rev Cient Acad Força Aérea. 2018;182-194.
5. Fernandes NA, Ramos PM, Borges GL, Rosa TA, Bessa CA. NATO – Kosovo Force. Prevalência da cárie dentária em militares portugueses. Rev Port Estomatol Med Dent Cir Maxilofac. 2017;58(S1):33.
6. Simecek JW, Diefenderfer KE. An evaluation of U.S. Navy Dental Corps classification guidelines. Mil Med. 2010;175:895–900.
7. Wojcik BE, Fedorowicz WS, Humphrey RJ, Colthirst PJ, Guerrero AC, Simecek JW, et al. Risk of dental disease, nonbattle injuries and severity of dental disease in deployed U.S. Army personnel. Mil Med. 2015;180:570-7.
8. Shetty K, Sindhu R, Manipal S, Prabu D, Mohan R, Bharathwaj VV. Aviation dentistry: is it an unexplored field of dentistry? A cross sectional study. J Aerosp Technol Manag. 2020;12:e2420.
9. National Academies of Sciences, Engineering, and Medicine. Nutrient composition of rations for short-term, highintensity combat operations. Washington, DC: The National Academies Press; 2006.
10. Pathak A, Saxena V, Jain M, Tiwari V, Sharva V, Upadhyaya S. Oral health related quality of life in relation to oral health status among residents in the surrounding areas of rural health training center attached to a medical college hospital. J Orofac Res. 2015;5:118–24.
11. Martins D, Botelho J, Júdice A, Proença L, Mendes JJ, Machado V. Prevalence of periodontitis and associated factors among Portuguese Air Force pilot cadets: a cross-sectional study. Front Public Health. 2025;13:1724111.
12. Azevedo L, Martins D, Fialho J, Veiga N. Oral health behaviors and dental caries in a sample of Portuguese militaries. Rev Port Estomatol Med Dent Cir Maxilofac. 2018;59:18–23.
13. Leggett H, Mitchell A, Csikar J, Vinall-Collier K, Douglas GVA. An exploration of the relationship between attitudes and experiences of prevention and oral health behaviours of the public within six European countries. BMC Oral Health. 2025;25:597.
14. Kawamura M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. J Hiroshima Univ Dent Soc. 1988;20(2):273–86.
15. Albuquerque T, Bernardo MF, Simão AM, Ferreira AS, Kawamura M, Okada M. Reprodutibilidade da versão portuguesa do Hiroshima University Dental Behavioural Inventory (HUDBI–versão portuguesa). Diferenças nas atitudes e comportamentos entre estudantes do 1.º e 3.º ano do curso de Higiene Oral. Rev Port Estomatol Med Dent Cir Maxilofac. 2011;52:125–32.
16. Albuquerque T. Atitudes, comportamentos e condições de saúde oral de estudantes universitários ao longo da sua vivência académica [tese]. Lisboa: Faculdade de Medicina Dentária da Universidade de Lisboa; 2013.
17. Almeida S, Albuquerque T, Bernardo M, Mendes S. Atitudes, comportamentos e estado de saúde oral de estudantes do 5.º ano de Medicina Dentária. Rev Port Estomatol Med Dent Cir Maxilofac. 2022;63:27–34.
18. Dias I, Albuquerque C, Cunha M, Dias A, Dias AR. Atitudes de saúde oral e comportamentos de risco em estudantes de enfermagem. Millenium. 2020;7(2):27–34.
19. Ferreira S, Albuquerque T, Bernardo M, Mendes S. Comportamentos, atitudes e estado de saúde oral dos alunos do 3.º ano da Faculdade de Medicina Dentária da Universidade de Lisboa. Rev Port Estomatol Med Dent Cir Maxilofac. 2018;59:205-14.
20. Fortes C, Mendes S, Albuquerque T, Bernardo M. Atitudes, comportamentos e estado de saúde oral dos alunos do 1.º ano da Faculdade de Medicina Dentária da Universidade de Lisboa. Rev Port Estomatol Med Dent Cir Maxilofac. 2016;57:236-46.
21. Mahdi SS, Sibilio F, Amenta F. Dental hygiene habits and oral health status of seafarers. Int Marit Health. 2016;67:9–13.
22. Cristóvão D, Machado C. Saúde oral nas unidades de saúde da força aérea [monografia]. Lisboa: Instituto Universitário Militar; 2022.
23. Khalilazar L, Khoshdel AR. Oral health profile in Iranian armed force: focusing on prevention strategies. J Arch Mil Med. 2016;4:e39275.
24. Levin L, Shenkman A. The relationship between dental caries status and oral health attitudes and behavior in young Israeli adults. J Dent Educ. 2004;68:1185–91.
25. Díaz‑Reissner C, Ávalos González D, Carabajal S, Quintana‑Molinas ME, Morel‑Barrios MI. Attitudes and behaviors related to oral health in young Paraguayan aspiring soldiers: a cross‑sectional study. Rev Cient Odontol (Lima). 2025;13:e226.
26. Komabayashi T, Kawamura M, Kim KJ, Wright FA, Declerck D, Goiás MdC, et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University Dental Behavioural Inventory (HUDBI) among final year dental students in 17 countries. Int Dent J. 2006;56:310–6.
27. Jones M, Lee JY, Rozier RG. Oral health literacy among adult patients seeking dental care. J Am Dent Assoc. 2007;138:1199–206.
28. Kutner M, Greenberg E, Jin Y, Paulsen C. The health literacy of America’s adults: results from the 2003 National Assessment of Adult Literacy. Washington (DC): National Center for Education Statistics, U.S. Dept of Education; 2006. NCES 2006‑423.
29. Ordem dos Médicos Dentistas. Barómetro da Saúde Oral 2024. Available from: https://www.omd.pt/content/uploads/2025/01/barometro-saude-oral-2024.pdf. Accessed 24 Jul 2025].
30. Werkhoven YAB, Dijkstra A, van der Wal H, Basic N, Loomans SA, van der Schans CP, et al. Promoting oral hygiene behavior in recruits in the Dutch Army. Mil Med. 2009;174:971–6.
31. Skec V, Macan JS, Susac M, Jokić D, Brajdić D, Macan D. Influence of oral hygiene on oral health of recruits and professionals in the Croatian Army. Mil Med. 2006;171:1006–9.
32. Senra MC. Caracterização de saúde oral numa amostra de militares da base naval de Lisboa [tese]. Lisboa: Instituto de Ciências da Saúde; 2015.
33. Norris JR, Irwin SP, Park J, Stephens RA, Moss ME, Weintraub JA. Risk indicators of urgent and extensive dental treatment needs in U.S. Air Force recruits. Mil Med. 2021;186:e194–202.
34. Rahmati F, Yaghoubi M. Oral health behaviors and community periodontal index among military staffs in Tehran, Iran. Open J Dent Oral Health. 2022;5:622.
35. Kovacević V, Milosavljević M, Rancić N, Daković D. Assessment of the periodontal health and community periodontal index in the Army of Serbia. Vojnosanit Pregl. 2015;72:953–60.
36. Rivera C. Essentials of recurrent aphthous stomatitis (Review). Biomed Rep. 2019;11:47–50.
37. Boschin F, Boutigny H, Delcourt‑Debruyne E. Maladies gingivales induites par la plaque. EMC–Dentisterie. 2004;1:462–80.
38. Immonen M, Anttonen V, Patinen P, Kainulainen MJ, Päkkilä J, Tjäderhane L, Oikarinen K. Dental traumas during the military service. Dent Traumatol. 2014;30:182–7.
Sónia Ferreira
E-mail address: soniaferreira@campus.ul.pt
CRediT authorship contribution statement
Sónia Ferreira: Conceptualisation, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft; Sónia Mendes: Conceptualisation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing; Mário Bernardo: Conceptualisation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Acknowledgments
The authors would like to thank Força Aérea Portuguesa for their availability and cooperation in distributing the study questionnaire
1646-2890/© 2026 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).