
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2025 | 66 (4) | 182-190
Original research
Social determinants and oral cancer mortality in Brazil: A 20-year analysis
Determinantes sociais e mortalidade por cancro oral no Brasil: Análise de 20 anos
a Federal University of Alagoas (UFAL), Maceió, Alagoas, Brazil
b State University of Bahia (UNEB), Salvador, Bahia, Brazil
c State University of Feira de Santana (UEFS), Feira de Santana, Bahia, Brazil
Alessandra Laís Pinho Valente Pires - lecavalent@hotmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 66
Issue - 4
Original research
Pages - 182-190
Go to Volume
Article History
Received on 24/02/2025
Accepted on 14/12/2025
Available Online on 30/12/2025
Keywords
Original Research
Social determinants and oral cancer mortality in Brazil: A 20-year analysis
Determinantes sociais e mortalidade por cancro oral no Brasil: Análise de 20 anos
Marília de Matos Amorim1 0000-0002-5224-4918
Daniel Deivson Alves Portella2 0000-0002-0315-9987
Alessandra Laís Pinho Valente Pires3,* 0000-0002-6848-8992
Carlos Alberto Lima da Silva3 0000-0003-3221-265X
Valéria Souza Freitas3 0000-0002-7259-4827
1 Federal University of Alagoas (UFAL), Maceió, Alagoas, Brazil
2 State University of Bahia (UNEB), Salvador, Bahia, Brazil
3 State University of Feira de Santana (UEFS), Feira de Santana, Bahia, Brazil
Article history:
Received 24 February 2025
Accepted 14 December 2025
Available online 31 December 2025
Abstract
Objectives: To analyze the association between social determinants and oral cancer mortality in Brazil from 1997 to 2017.
Methods: An ecological panel data study based on oral cancer mortality. The social determinants were represented by the income ratio, the Human Development Index, the Gini coefficient, the illiteracy rate, the average household income, the rate of people living below the poverty line, and the percentage of the black population. A descriptive analysis of mortality rates was performed, assessing heterogeneity across space and time and characterizing social determinants. The statistical association was verified using a multivariate negative binomial regression model (selected to account for overdispersion observed in the initial Poisson regression).
Results: In states where there was an increase in income inequality and illiteracy rate (p<0.001), there was a reduction in mortality rates (p=0.03). In states where there was na increase in average household income per capita (p<0.001), the rate of people living below the poverty line (p<0.001), and the percentage of the black population (p=0.03), there was na increase in mortality rates from oral cancer.
Conclusions: There are positive and negative associations between social determinants and oral cancer mortality rates. (Rev Port Estomatol Med Dent Cir Maxilofac. 2025;66(4):182-190)
Keywords: Mortality, Mouth Neoplasms,Social determinants of health
Resumo
Objetivos: Analisar a associação entre determinantes sociais e a mortalidade por cancro oral no Brasil de 1997 a 2017.
Métodos: Estudo ecológico de dados em painel realizado a partir da mortalidade por cancro oral. Os determinantes sociais foram representados pela razão de renda, índice de desenvolvimento humano, coeficiente de Gini, taxa de analfabetismo, renda média domiciliar, índice de pessoas que vivem abaixo da linha da pobreza e percentagem da população preta (classificação IBGE). Foi realizada a análise descritiva das taxas de mortalidade, avaliada a sua heterogeneidade em função do espaço e do tempo e caracterizados os determinantes sociais. A associação estatística foi verificada utilizando um modelo multivariado de regressão binomial negativa (em substituição do modelo de Poisson para corrigir a sobredispersão).
Resultados: Nos estados em que houve aumento da desigualdade de renda e taxa de analfabetismo (p<0,001), houve redução das taxas de mortalidade (p=0,03). Nos estados em que houve aumento da renda média domiciliar per capita (p<0,001), do índice de pessoas que vivem abaixo da linha de pobreza (p<0,001) e da porcentagem da população preta (p=0,03), houve aumento das taxas de mortalidade por cancro oral.
Conclusões: Existem associações positivas e negativas entre determinantes sociais e as taxas de mortalidade por cancro oral.
Palavras-chave: Mortalidade, Neoplasias orais,Determinantes sociais da saúde
Introduction
According to the World Health Organization (WHO), head and neck cancers account for between 0.5% and 2% of all malignant diseases. Data from the International Agency for Research on Cancer (IARC) revealed a crude incidence rate for Latin America and the Caribbean in 2022 of 2.9 per 100,000 inhabitants and a mortality rate for the same year of 1.3 deaths per thousand inhabitants.1 In turn, the National Cancer Institute (INCA) indicates that Brazil has the highest incidence of the disease in South America, with an estimated 15,100 new cases of oral cancer, 10,900 in men and 4,200 in women, per year in the three-year period 2023-2025.1, 2
The etiology of oral cancer is multifactorial, occurring from the interaction of genetic, environmental, and, above all, lifestyle-related factors, especially the consumption of tobacco and alcoholic beverages.3 Other factors include a family history of cancer, diet, sun exposure (lip cancer), and some viral infections, such as human papillomavirus (HPV) and Epstein-Barr virus.4, 5
The concept of social determination has been proposed to investigate how diseases behave in a given population and to explain how distribution occurs unevenly in some situations.
Thus, the social determinants of health highlight specific characteristics of the social context that affect health, as well as how social conditions translate these impacts on health.6, 7
According to Dahlgren and Whitehead’s theoretical model from 1991,8 social inequalities in health are the result of interactions between different levels of conditions. The model distributes the social determinants of health into five layers: two more proximal layers, two intermediate layers, and a final distal layer, the macro-determinants.
Social determinants may be associated with both the occurrence of oral cancer and its mortality. A systematic review by Dourado-Martins et al.9 revealed that variables such as education, family income, occupation, geographical area, social marginalization, longevity, and the Human Development Index (HDI) were related to the occurrence of oral cancer. Race/ethnicity may also be related to the occurrence and mortality of the disease, since the black population is mainly concentrated in peripheral areas, where they experience other social inequalities and greater barriers to accessing health services.
However, some aggregate studies investigating the relationship between disease mortality and social and economic indicators have yielded controversial results. 10 - 12
In Brazil, the highest oral cancer mortality rates are in the South and Southeast, which are regions with better social indicators. 13, 14 The most recent data from the Ministry of Health’s Mortality Information System (SIM-MS), together with the Brazilian Institute of Geography and Statistics (IBGE) population data, revealed a crude mortality rate of 3.4 deaths per 100,000 men and 1.1 deaths per 100,000 women in 2022, with this rate being higher in the South region at 2.7 and the Southeast region at 2.4.15 Additionally, some aggregate studies have shown an association between better social indicators and higher mortality rates from the disease.12, 16
Taking into account the high rates of oral cancer mortality in Brazil, the polarization of the highest rates in regions with better social and economic indicators, as well as the controversies in the literature on the subject, ecological studies that evaluate social determinants and mortality from the disease can help visualize the rates in different states, verify their behavior over time, and analyze the possible associated social determinants. The results can contribute to interventions and strategies to prevent, control, and reduce mortality from the disease.17 Thus, the aim of this study is to assess the association between social determinants and the oral cancer mortality rate in Brazil between 1997 and 2017.
Material and methods
This was an ecological study using a panel data set in Brazil, with all states and the Federal District as the unit of analysis.
The study object was the oral cancer mortality rate, classified according to the 10th International Classification of Diseases(ICD-10) C00, C01, C02, C03, C04, C05, C06, C07, C08, C09, and calculated per 100,000 inhabitants. Mortality data were obtained from the SIM/MS, and the number of inhabitants was obtained from the latest IBGE census and intercensal estimates for the years studied.
The social determinants were represented by the income ratio (number of times the aggregate income of the top fifth of the income distribution (richest 20%) is greater than the income of the bottom fifth (poorest 20%) of the population), the Gini coefficient (measures the degree of income concentration), the HDI (index that summarizes the average performance of a territory in three basic dimensions of human development: longevity, education and income), the illiteracy rate (proportion of people aged 15 and over who cannot read and write at least a simple note), the average household income (sum of the monthly income, expressed in reais (R$), of all residents in the household divided by the total number of residents in the household), the rate of people living below the poverty line (index of people who have less than US$1.90 per day), and the percentage of the black population (proportion of the population declared black). All values were collected from the Atlas of Human Development in Brazil by the United Nations Development Program (UNDP) and the Continuous National Household Sample Survey (PNAD) by the IBGE and the Institute for Applied Economic Research (IPEA).
A descriptive analysis of the time series of oral cancer mortality rates was carried out across the different units of analysis to assess heterogeneity by space and time and characterize oral cancer mortality rates and their social determinants.
The statistical association between oral cancer mortality rates and social determinants was evaluated using a multivariate negative binomial regression model, which was selected to account for overdispersion observed in the initial Poisson regression.
The Hausman test was used to assess whether the estimators in the random effects model are equal to those in the fixed effects model, resulting in the use of the fixed effects model.
In order to quantitatively interpret the effect of social determinants in determining the risk of oral cancer mortality, the exponential regression model coefficient for each predictor was multiplied by “n” times to make the association with the outcome easier to understand. To check for collinearity among the variables, the variance inflation factor (VIF) was calculated, with results for all variables (maximum value of 3.07) well below the cut-off point (10) suggested by the literature.18
Microsoft Office Excel 2013 for Windows and STATA/SE 14 were used to build the database and perform the statistical analysis. The databases used in this research are open-access and do not contain data that would allow the research subjects to be identified.
Results
Between 1997 and 2017, there were 64,526 deaths from oral cancer throughout Brazil. Figure 1 shows the time series of oral cancer mortality rates in the different states and the Federal District. Graphically, the rates varied across most states, with São Paulo showing the greatest stability over time.
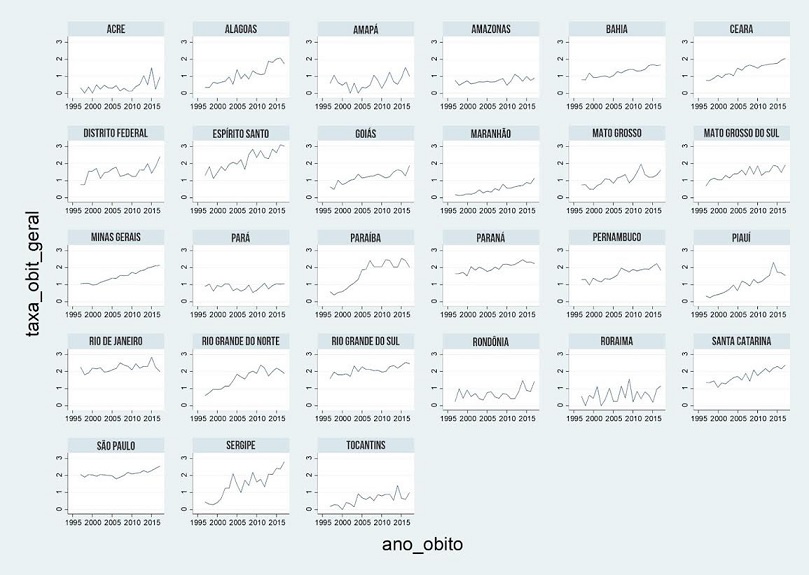
Figure 1. Oral cancer mortality rate, according to Brazilian states, 1997 to 2017.
Source: Mortality Information System, Brazilian Institute of Geography and Statistics (IBGE), 1997-2017.
The heterogeneity and the average mortality rate by space are shown in Figure 2. The highest mortality rates were seen in the state of Espírito Santo, followed by Rio de Janeiro and Sergipe.
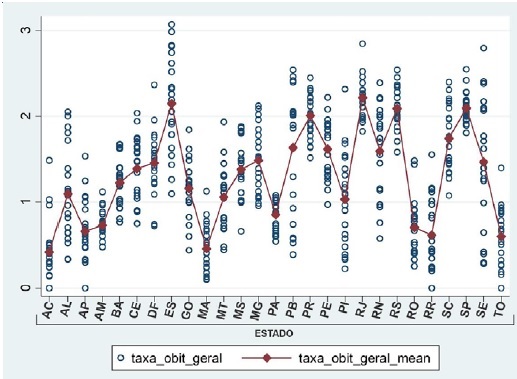
Figure 2. Heterogeneity of the average oral cancer mortality rate in Brazilian states, 1997 to 2017.
Source: Mortality Information System, Brazilian Institute of Geography and Statistics (IBGE), 1997-2017.
Figure 3 shows the spatial distribution of average oral cancer mortality rates in Brazil from 1997 to 2017. The highest average rates were observed in the states of Rio de Janeiro, Espírito Santo, Rio Grande do Sul, and São Paulo.
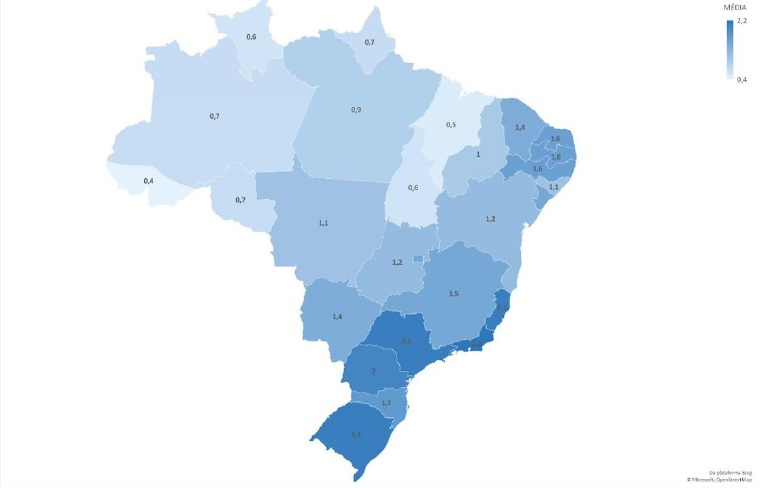
Figure 3. Spatial distribution of average oral cancer mortality rates in Brazil, 1997 to 2017.
Source: Mortality Information System, Brazilian Institute of Geography and Statistics (IBGE), 1997-2017.
The heterogeneity and average mortality rates from oral cancer over time are shown in Figure 4. In general, rates increased over time. The highest rate was in 2016, followed by 2017, both in the state of Espírito Santo.
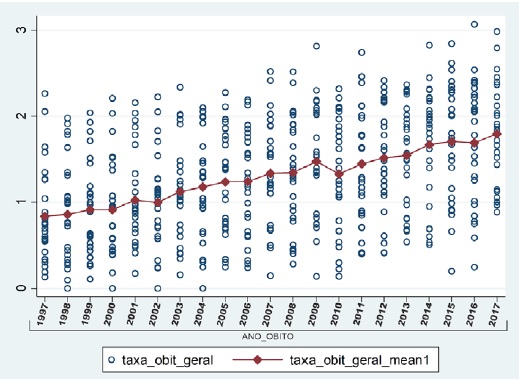
Figure 4. Heterogeneity of the average oral cancer mortality rates between 1997 and 2017 in the states of Brazil.
Source: Mortality Information System, Brazilian Institute of Geography and Statistics (IBGE), 1997-2017.
Table 1 shows the characterization of oral cancer mortality rates and social determinants by Brazilian state. For descriptive analysis, the states were divided into two groups based on their highest and lowest average mortality rates. The six states with the highest average oral cancer mortality rates were all in the Southeast and South: Rio de Janeiro, Espírito Santo, Rio Grande do Sul, São Paulo, Paraná, and Santa Catarina. The six states with the lowest average rates were all in the North and Northeast, mainly in the North: Acre, Maranhão, Roraima, Tocantins, Amapá, and Amazonas. The other states and the Federal District had intermediate average mortality rates.
Table 1. Characterization of the oral cancer mortality rates and social determinants by Brazilian states, 1997 to 2017.
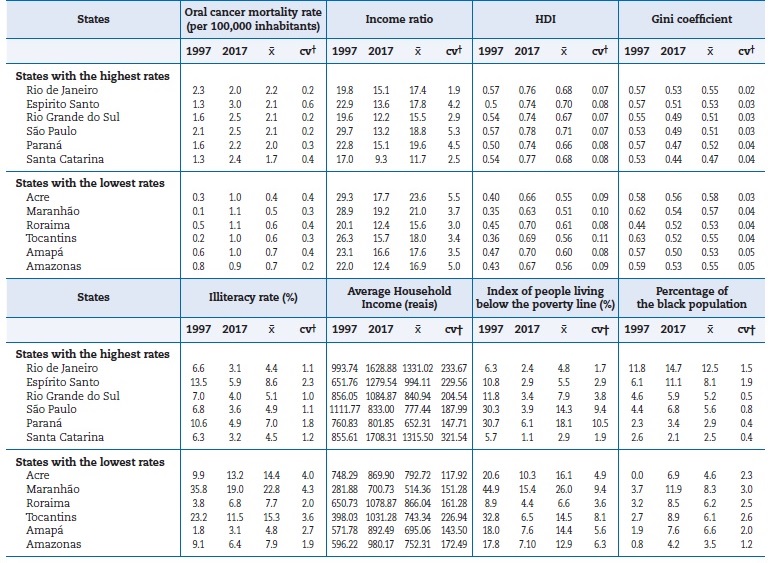
Source: Mortality Information System, United Nations Development Program (UNPD) and the Continuous National Household Sample Survey
(PNAD) of the Brazilian Institute of Geography and Statistics (IBGE) and the Institute of Applied Economic Research (IPEA).
Data processed by the authors.
HDI – Human Development Index; † Coefficient of variation (cv=standard deviation)
Table 2 shows the multivariate negative binomial regression model using fixed effects to assess the association between social determinants and the oral cancer mortality rate
across Brazilian states between 1997 and 2017. The results showed statistical significance for the determinants of income ratio (p=0.033), illiteracy rate (p<0.001), average household income (p<0.001), index of people living below the poverty line (p=0.001), and percentage of the black population (p=0.034).
Table 2. Multivariate negative binomial regression model (fixed effects) for the association between oral cancer mortality rate and social determinants in Brazil, from 1997 to 201
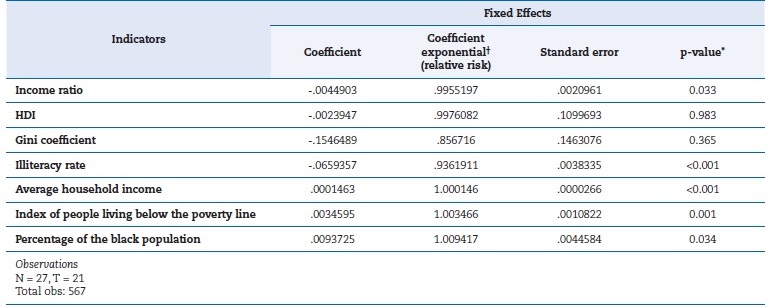
Source: Mortality Information System, United Nations Development Program (UNDP) and the Continuous National Household Sample Survey
(PNAD) of the Brazilian Institute of Geography and Statistics (IBGE) and the Institute of Applied Economic Research (IPEA), 1997-2017.
Data processed by the authors.
† The coefficient exponential was multiplied by “n” times for the quantitative interpretation of the effect of each indicator on the oral cancer
mortality rate; *Adjusted for the other variables in the model.
However, some determinants showed an inverse relationship with the mortality rate in terms of social coherence. Regarding the income ratio, in a given state, a 10% increase in the income ratio was associated with a 96% decrease in the oral cancer mortality rate. For the illiteracy rate, in states where the rate increased by 10%, the oral cancer mortality rate decreased by 52%. With regard to average household income, in states with a 200 reais increase, the mortality rate increased by 3%. However, when the percentage of people living below the poverty line increased by 10%, the mortality rate rose by 4%. In addition, in the states where there was a 15% increase in the percentage of the black population, there was also a 15% increase in the oral cancer mortality rate.
Discussion
Although the highest oral cancer mortality rates are observed in the South and Southeast regions, the trend shows higher growth in the North and Northeast.19 In the study by Souza19 on the period 1996−1998, the highest average rates were described in Rio Grande do Sul, Paraná, Santa Catarina, Rio de Janeiro, São Paulo, Amapá, Tocantins, and Alagoas. These results show that the entire Southern region had higher average mortality rates.
However, in the 2014−2016 period, the highest average rates were in Rio Grande do Norte, Paraíba, Pernambuco, Alagoas and Sergipe, Rio de Janeiro, Espírito Santo, Santa Catarina, and Paraná, most of which were in the Northeast region.
The study by Perea et al.14 revealed that the Northeast had one of the lowest average coefficients for the period, but with an average annual increase in mortality of 6.9%. The Southeast, on the other hand, had the second-highest average coeficiente but was the only region to see a reduction in mortality rates.
This study did not calculate the trend or the annual percentage variation in mortality rates. According to Borges et al.,16 who studied the proportional mortality rate for oral cancer in Brazil, regions with better socioeconomic indicators are more likely to develop chronic-degenerative diseases because, according to the IBGE, they have better demographic indicators for life expectancy at 60 years of age and a higher proportion of elderly people in the population.
In addition, the underreporting of deaths in some states in the North and Northeast must also be taken into account.
During the period studied, Brazil underwent significant changes in terms of oral health care. Significant changes in oral health have taken place since 2000, with the expansion of oral health in primary care and the publication of the National Oral Health Policy (PNSB) guidelines and the establishment of a network of care for the prevention and control of the disease, as well as care for people with oral cancer.20 - 23 However, there was no decline in the average mortality rates from oral cancer over the studied period. In the time series, the only reduction observed was from 2009 to 2010. On the other hand, a study by Cunha, Prass, and Hugo24 found an association between the implementation of this policy and oral and oropharyngeal cancer mortality rates in Brazil. The study found that the expansion of primary dental care coverage and the number of Dental Specialty Centers were associated with a reduction in oral and oropharyngeal cancer mortality rates in Brazil.
Thus, the increase in mortality rates over time in this study may reflect increased access to health services for disease treatment and, consequently, greater notification of deaths from the disease. Furthermore, the long-term benefits of health policies should be considered.14
In this study, the social determinants that were statistically significant were: income ratio, illiteracy rate, average household income, index of people living below the poverty line, and percentage of the black population.
The income ratio is an indicator of economic inequality, and the results of this study show an inverse relationship: the greater the inequality, the lower the oral cancer mortality rates. Other studies have shown an inverse relationship between an economic indicator and the oral cancer mortality rate.16,25 The study by Borges et al.16revealed a proportional relationship between mortality from the disease and the specific HDI for income and average household income per capita.
Assis25 also found an association with per capita income, showing that higher per capita income is associated with higher oral cancer mortality rates. In the present study, an increase in per capita income was also associated with higher mortality rates. However, the study by Sakamoto et al.11 showed a significant decrease in mortality rates as average incomes increased.
Another statistically significant social determinant was the illiteracy rate, for which an increase was associated with a decrease in the mortality rate. This social determinant was also studied by Petti and Scully.26 According to those authors, there is a positive correlation between this variable and the oral cancer mortality rate, indicating that the higher the illiteracy rate in countries, the higher the mortality rates, unlike the findings of this study.
The increase in the number of people living below the poverty line in this study was associated with an increase in mortality rates. For some authors, the relationship between poverty and oral cancer mortality can be explained by greater exposure to the main risk factors for the disease and less availability and access to diagnosis and early treatment of the disease in less favored regions.27, 28
In this study, an increase in the percentage of the black population was associated with an increase in oral cancer mortality rates. Race/ethnicity can be considered a social determinant related to sociodemographic characteristics; however, it can also be related to living and socioeconomic conditions, the social and educational environment, and influences on behaviors and the construction of social networks. Furthermore, race/ethnicity is considered one of the determinants of social inequality in cancer, which is complexly related to social class, reflecting the distribution of power between groups in a society.8 Other studies have looked at this determinant and its relationship with oral cancer mortality.10, 29, 30 The study by Molina et al.29 showed that head and neck cancers have a high overall mortality rate with a disproportionate impact on African-American and poor patients. The authors revealed that the high disparities by race and socioeconomic status are not fully explained by demographics, comorbid conditions, or undertreatment.
Although oral cancer in Brazil mainly affects white people, Antunes et al.10 through an ecological study carried out in São Paulo, revealed an increase in rates for the black population and stabilization for the white population. The study points out that oral cancer mortality in the black population almost doubled during the study period and exceeded mortality in the white population in almost all categories.
The limitations of this study must be considered: trends in rates were not calculated, and mortality rates were not standardized by sex, age, or anatomical site. Furthermore, ecological studies are subject to the ecological fallacy bias, meaning the results presented cannot be inferred at the individual level. Other aspects to consider include the fact that this is a study using secondary, outdated data, which makes its validity dependente on the reliability of the sources. Therefore, we suggest conducting new, more up-to-date national studies to expand knowledge on the social determinants and oral cancer mortality in Brazil and thus support the development of effective prevention policies. Furthermore, other data analysis approaches are suggested, including standardizing rates, accounting for other determinants, and better controlling for confounding factors.
Conclusions
The determinants that showed a statistical association with the mortality rate were the income ratio, illiteracy rate, average household income per capita, index of people living below the poverty line, and percentage of the black population. In states where there was an increase in income inequality and the illiteracy rate, there was a reduction in mortality rates, and in states where there was an increase in average household income per capita, the index of people living below the poverty line, and the percentage of the black population, there was na increase in oral cancer mortality rates.
References
1. Globocan: Estimated Cancer Incidence. Mortality and Prevalence Worldwide in 2022. International Agency for Research on Cancer; 2022. Lyon: IARC; 2022. Available from: https://gco.iarc.fr/today/home. Accessed 3 July, 2024.
2. Ministério da Saúde do Brasil, Instituto Nacional de Câncer. Estimativa 2023: Incidência de Câncer no Brasil. Rio de Janeiro: INCA 2022. Available from: https://www.inca.gov.br/publicacoes/livros/estimativa-2023-incidencia-de-cancer-nobrasil. Accessed: 3 July, 2024.
3. Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45:301‑8.
4. Petti S. Lifestyle risk factors for oral cancer. Oral Oncol. 2009;45:340‑50.
5. Young D, Xiao CC, Murphy B, Moore M, Fakhry C, Day TA. Increase in head and neck cancer in younger patients due to human papillomavirus (HPV). Oral Oncol. 2015;51:727‑30.
6. Costa SM, Adelário AK, Vasconcelos M, Abreu MHNG. Modelos explicativos da cárie dentária: do organicista ao ecossistêmico. Pesqui Bras Odontopediatria Clín Integr. 2012;12:285-91.
7. Bueno RE, Moysés ST, Bueno PAR, Moysés SJ. Determinantes sociais e saúde bucal de adultos nas capitais do Brasil. Ver Panam Salud Publica. 2014;36:17-23.
8. Dahlgren G, Whitehead M. Policies and strategies to promote social equity In health. Stockholm: Institute For Future Studies, 1991.
9. Dourado JM, Oliveira JAM, Freitas VS, Araújo TM. Determinantes sociais de saúde e a ocorrência de câncer oral: uma revisão sistemática de literatura. Rev Salud Pública. 2014;16:786-98.
10. Antunes JLF, Toporcov TN, Biazevic MGH, Boing AF, Bastos JL. Gender and racial inequalities in trends of oral cancer mortality in São Paulo, Brazil. Rev Saúde Pública.2013;47:470-8.
11. Sakamoto AJ, Brizon VSC, Bulgareli JV, Ambrosano GMB, Hebling E. Influência dos índices socioeconômicos municipais nas taxas de mortalidade por câncer de boca e orofaringe em idosos no estado de São Paulo. Rev Bras Epidemiol. 2019;22:e190013.
12. Freire AR, Freire DEWG, Araújo ECF, Carrer FCA, Pucca Júnior GA, Sousa SA, et al. Socioeconomic indicators and economic investments influence oral cancer mortality in Latin America. BMC Public Health. 2021;21:1-6.
13. Tavani A, Gallus S, La Vecchia C, Talamini R, Barbone F, Herrero R, et al. Diet and risk of oral and pharyngeal cancer: an Italian case–control study. Eur J Cancer Prev. 2001;10:191-5.
14. Perea LME, Peres MA, Boing AF, Antunes JLF. Tendência de mortalidade por câncer de boca e faringe no Brasil no período 2002-2013. Rev Saúde Pública. 2018;52:10.
15. Ministério da Saúde do Brasil. Sistema de Informação Sobre Mortalidade. Available from: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sim/cnv/obt10uf.def. Accessed 3 July, 2024.
16. Borges DMDL, Sena MFD, Ferreira MÂF, Roncalli ÂG. Mortalidade por câncer de boca e condição sócio-econômica no Brasil. Cad Saude Publica. 2009;25:321-7.
17. Moreira RDS, Nico LS, Tomita NE. A relação entre o espaço e a saúde bucal coletiva: por uma epidemiologia georreferenciada. Cienc Saude Coletiva. 2007;12:275-84.
18. Montgomery DC, Peck EA, Vining GG. Introduction to linear regression analysis. John Wiley & Sons, 2021.
19. Souza FCD. Mortalidade por câncer de cavidade bucal e orofaringe nos estados brasileiros: uma análise de tendência [dissertation]. São Paulo: Universidade de São Paulo, Faculdade de Saúde Pública; 2021.
20. Ministério da Saúde do Brasil. Portaria n.º 1444/GM Em 28 de dezembro de 2000. Estabelece incentivo financeiro para a reorganização da atenção à saúde bucal prestada nos municípios por meio do Programa de Saúde da Família, 2000.
21. Ministério da Saúde do Brasil. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Diretrizes da Política Nacional de Saúde Bucal. Brasília: Ministério da Saúde, 2004. Available from: http://189.28.128.100/dab/docs/publicacoes/geral/diretrizes_da_politica_nacional_de_saude_bucal.pdf. Accessed 3 July, 2024.
22. Ministério da Saúde do Brasil. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. A saúde bucal no Sistema Único de Saúde. Ministério da Saúde, Secretaria de Atenção à Saúde, 2018. Available from: http://bvsms.saude.gov.br/bvs/ publicacoes/saude_bucal_sistema_unico_saude.pdf. Accessed 3 July, 2024.
23. Ministério da Saúde do Brasil. Portaria nº 1.444/GM, de 28 de dezembro de 2000. Estabelece incentivo financeiro para a reorganização da atenção à saúde bucal prestada nos municípios por meio do Programa de Saúde da Família. Brasília: Ministério da Saúde; 2000 Available from: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2000/prt1444_28_12_2000.html. Accessed 3 August, 2025.
24. Cunha ARD, Prass TS, Hugo FN. Mortality from oral and oropharyngeal cancer in Brazil: impact of the National Oral Health Policy. Cad Saude Publica. 2019;35:e00014319.
25. Assis APB. Distribuição espacial da mortalidade por câncer de boca e fatores de risco para o câncer de língua no estado da Bahia [mater dissertation]. Salvador: Universidade Federal da Bahia – Faculdade de Medicina da Bahia; 2013.
26. Petti S, Scully C. Determinants of oral cancer at the national level: just a question of smoking and alcohol drinking prevalence? Odontology. 2010;98:144-52.
27. Weitkunat R, Sanders E, Lee PN. Meta-analysis of the relation between European and American smokeless tobacco and oral cancer. BMC Public Health. 2007;7:334.
28. Turati F, Garavello W, Tramacere I, Pelucchi C, Galeone C, Bagnardi V et al. A meta-analysis of alcohol drinking and oral and pharyngeal cancers: results from subgroup analyses. Alcohol Alcohol. 2013;48:107-18.
29. Molina MA, Cheung MC, Perez EA, Byrne MM, Franceschi D, Moffat FL, et al. African American and poor patients have a dramatically worse prognosis for head and neck cancer: na examination of 20,915 patients. Cancer. 2008;113:2797-806.
30. Dantas TS, Silva PGB, Sousa EF, da Cunha MDP, de Aguiar ASW, Costa FWG. Influence of educational level, stage, and histological type on survival of oral cancer in a Brazilian population: a retrospective study of 10 years observation. Medicine (Baltimore). 2016;95:e2314.
Alessandra Laís Pinho Valente Pires
E-mail address: lecavalent@hotmail.com
CRediT authorship contribution statement
Marília de Matos Amorim: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. Daniel Deivson Alves
Portella: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. Alessandra Laís Pinho Valente Pires: Conceptualization, Writing – original draft, Writing – review & editing. Carlos Alberto Lima da Silva: Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. Valéria Souza Freitas: Conceptualization, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
1646-2890/© 2025 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).