
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2025 | 66 (4) | 175-181
Original research
Prevalence of orthodontically induced inflammatory root resorption (OIIRR) associated with distal movement of the maxillary teeth with mini-implants – A preliminary CBCT cohort study
Prevalência de reabsorção radicular inflamatória induzida ortodonticamente (RRIO) associada à movimentação distal dos dentes maxilares com mini-implantes – Um estudo preliminar de coorte com TCFC
a Department of Orthodontics and Dentofacial Orthopedics, Saveetha Dental College & Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
b Department of Oral Medicine, Saveetha Dental College & Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
A. Sumathi Felicita - sumifeli@hotmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 66
Issue - 4
Original research
Pages - 175-181
Go to Volume
Article History
Received on 10/05/2025
Accepted on 30/11/2025
Available Online on 30/12/2025
Keywords
Original Research
Prevalence of orthodontically induced inflammatory root resorption (OIIRR) associated with distal movement of the maxillary teeth with mini-implants – A preliminary CBCT cohort study
Prevalência de reabsorção radicular inflamatória induzida ortodonticamente (RRIO) associada à movimentação distal dos dentes maxilares com mini-implantes – Um estudo preliminar de coorte com TCFC
A. Sumathi Felicita1,* 0000-0003-2002-0140
T.N. Uma Maheswari2 0000-0002-2366-2336
1 Department of Orthodontics and Dentofacial Orthopedics, Saveetha Dental College & Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
2 Department of Oral Medicine, Saveetha Dental College & Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
Article history:
Received 19 May 2025
Accepted 30 November 2025
Available online 24 December 2025
Abstract
Objectives: To investigate the prevalence of orthodontically induced inflammatory root resorption (OIIRR) during distal movement of the entire maxillary dentition with mini-implants using cone-beam computed tomography.
Methods: A total of 224 teeth from 16 patients were evaluated. Distal movement of the maxillary teeth was performed on 0.018”x0.025” stainless-steel wire in 0.022 slot using mini‑implants. 200 grams of force were placed from mini-implants to attachments placed bilaterally in the anterior region to distalize the entire maxillary dentition. The roots of all the maxillary teeth were assessed on cone-beam computed tomography scans taken before and six months after distal movement of the maxillary teeth to determine the presence of OIIRR. Descriptive statistics were done to check the frequency and percentage of distribution of OIIRR.
Results: The percentage of distribution of OIIRR in the maxillary arch was highest in the right first permanent molar (68.8%), followed by the right central incisor (56.3%), the left and right second permanent molars (50% and 43.8%), the right central and lateral incisors and left permanent second molar (43.8%), the left first premolar (25%), the right second premolar (18.3%), and the first premolar and the canines of both sides (12.5%). Only the maxillary left second premolar did not have any evidence of OIIRR (0%).
Conclusions: The presence of OIIRR during distal movement of the maxillary teeth was very high, was greater in the posterior teeth compared to the anterior teeth, and was rarer in the premolar region. (Rev Port Estomatol Med Dent Cir Maxilofac. 2025;66(4):175-181)
Keywords: Cone-beam computed tomography, Orthodontics, Root resorption,Tooth
Resumo
Objetivos: Investigar a prevalência de reabsorção radicular inflamatória induzida ortodonticamente (RRIIO) durante a movimentação distal de toda a arcada dentária superior com mini-implantes, utilizando tomografia computadorizada de feixe cónico.
Métodos: Um total de 224 dentes foram avaliados em 16 pacientes. O movimento distal dos dentes maxilares foi realizado com fio de aço inoxidável de 0,018”x0,025” em slot 0,022 usando mini-implantes. Aplicou-se uma força de 200 gramas dos mini-implantes aos attachments colocados bilateralmente na região anterior para distalizar toda a dentição maxilar. As raízes de todos os dentes maxilares foram avaliadas em tomografias computadorizadas de feixe cónico realizadas antes e seis meses após o movimento distal dos dentes maxilares para determinar a presença de RRIIO. Efetuaram-se estatísticas descritivas para verificar a frequência e a percentagem de distribuição da RRIIO.
Resultados: A percentagem de distribuição de RRIIO na arcada superior foi maior no primeiro molar permanente direito (68,8%), seguindo-se o incisivo central direito (56,3%), os segundos molares permanentes esquerdo e direito (50% e 43,8%), os incisivos central e lateral direitos e o segundo molar permanente esquerdo (43,8%), o primeiro pré-molar esquerdo (25%), o segundo pré-molar direito (18,3%), e o primeiro pré-molar e os caninos de ambos os lados (12,5%). Apenas o segundo pré-molar superior esquerdo não apresentou evidência de RRIIO (0%).
Conclusões: A presença de RRIIO durante a movimentação distal dos dentes superiores foi muito elevada, sendo maior nos dentes posteriores do que nos anteriores e menor na região dos pré-molares.
Palavras-chave: Tomografia computadorizada de feixe cónico,Ortodontia, Reabsorção radicular, Dente
Introduction
Orthodontically induced inflammatory root resorption (OIIRR) occurs during orthodontic treatment as an inflammatory response to biologic and mechanical factors,1 - 3 and results in permanent root-length reduction. Genetic and systemic factors, calcium and vitamin D deficiency, age, sex, habits, anomalies of the position and number of teeth, dental trauma, and endodontic treatment can predispose to OIIRR.1 - 3 The orthodontic treatment itself can predispose a tooth to OIIRR. It may be related to factors such as type of malocclusion, rectangular arch wires, Class II elastics, anterior vertical elastics, Le-Fort I osteotomy, proximity to the palate, type of tooth movement, direction of force, presence of impacted teeth, and treatment mechanics employed.1 - 3 Although there is abundant literature on apical root resorption due to orthodontic treatment, OIIRR associated with the distal movement of all the maxillary teeth due to mini-implants has not been evaluated in the literature.
Distal movement of the maxillary teeth involves movement of the entire maxillary dentition from the central incisor to the maxillary second molar with mini-implants on both sides. In conventional methods of space closure, the anterior segment is the active unit and moves with the application of force, while the posterior segment serves as the anchorage unit. In turn, distal movement of the maxillary teeth envolves movement of the entire maxillary arch backward when subjected to orthodontic force with mini-implants placed at several sites, such as the infrazygomatic region,4 the buccal interradicular region between the second premolar and first permanent molar,5 - 8 or the palatal aspect of the maxilla.9, 10 It is effective in treating cases with mild-to-moderate archlength tooth size discrepancy with reduced axial inclination of the maxillary anterior teeth, molar intrusion, and reduction in overjet and overbite.4 - 10 This will correct an end-on/Class II molar relation to a Class I molar relation. In patients with Class I molar relation, concomitant distalization of the mandibular arch is required to maintain that relation. The distally applied force may result in unwanted side effects on the tooth, such as OIIRR, alveolar bone dehiscence, or tooth mobility. OIIRR may be associated with loss of vitality of the tooth, alteration of crown-root ratio, increase in relapse tendency, and, in extreme cases, loss of the tooth.
The identification of OIIRR and bone dehiscence requires radiographic evaluation, such as an orthopantomogram or na intraoral periapical radiograph. The anterior teeth may not be clearly visible on an orthopantomogram and may require na intraoral periapical radiograph of the particular tooth. However, intraoral periapical radiographs may not be beneficial for visualizing several teeth across different quadrants. Also, these radiographs provide a two-dimensional view of the maxillary teeth and may be affected by overlap from surrounding structures. A cone-beam computed tomography (CBCT) may be beneficial in such situations and offers a three-dimensional view of the maxillary arch.
CBCT scan offers a quantitative assessment of structures without the image magnification that occurs with conventional radiographs.11 The measurements are not influenced by a change in the orientation of the head.12 It also allows for three-dimensional visualization of the particular structure as compared to two-dimensional imaging with radiographs.
Hence, the present study was conducted to evaluate the presence of OIIRR with CBCT in patients undergoing orthodontic treatment involving distal movement of the entire maxillary arch with mini-implants. The aim of this study was to evaluate the frequency and percentage of teeth exhibiting OIIRR after distal movement of the entire maxillary dentition using mini-implants.
Material and methods
This study was a preliminary cohort study. The study was approved by the scientific board of our university with reference number SRB/SDC/FACULTY/20/ORTHO/04. It was further approved by the ethical board of our university with reference number IHEC/SDC/FACULTY/20/ORTHO/04.
Patients undergoing distal movement of the maxillary teeth with mini-implants requiring correction of mild-to-moderate arch-length tooth size discrepancy were selected. The inclusion criteria were healthy young individuals aged 15 years or older, of both sexes, without systemic diseases or a recente history of illness, and with a full complement of teeth except the third molars. Patients with severe skeletal discrepancy (skeletal Class II malocclusion with an ANB >6°), periodontal disease, and previous orthodontic treatment or temporomandibular disease were excluded from the study.
After a detailed explanation of the procedure, informed written consent was obtained from all patients who matched the inclusion criteria and agreed to participate. The sample size was calculated based on the average percentage of root resorption observed across all teeth during fixed appliance treatment, as reported in an earlier study.13 The sample size for prevalence studies such as the current study is calculated using the formula n= Z2 P(1-P)/d2 where n is the sample size, Z is the statistic corresponding to the level of confidence, P is the expected prevalence based on earlier studies, and d is the precision and corresponds to the effect size.14 In the presente study, the level of significance was set at 0.5 with a 95% confidence interval. The expected prevalence was 82% based on the earlier study,13 and the precision was 0.05. A total of 225 teeth were required to maintain an existing OIIRR prevalence of 82%. Eighteen patients and 252 teeth were selected for the study according to the inclusion and exclusion criteria. Two patients dropped out during the course of treatment for various reasons. All the teeth from the maxillary second molar to the central incisor on both sides were evaluated in 16 patients: six males and ten females. A total of 224 teeth and 338 roots were evaluated in the present study. Of the 16 patients, six had na Angle’s Class I molar relation, and ten patients had an end-on molar relation on a Class I skeletal base. In patients with Angle’s Class I molar relation, the mandibular arch was also distalized with mini-implants. The mean distalization was 1.77±1.12mm on the left side and 1.33±1.01mm on the right side over a six-month period.
Fixed orthodontic treatment was performed with 0.022 MBT bracket prescription (3M Unitek) bonded on the maxillary and mandibular dentition. The sequence of arch wire was 0.016” nickel-titanium wire, 0.016” x 0.022” stainless-steel wire, 0.017” x 0.025” stainless-steel wire, and 0.018” x 0.025” stainless-steel wire (3M unitek). After initial leveling and aligning, distal movement of the maxillary dentition was initiated in the maxillary arch on the 0.018” X 0.025” stainless-steel wire.
Stainless-steel mini-implants (1.2 X 8mm) (Orlus mini-implants, Ortholution, Seoul, Korea) were placed bilaterally at the mucogingival junction between the maxillary second premolar and the maxillary first permanent molar using a stent.15 The distal movement of the maxillary teeth was done with 200 grams of distalizing force applied with pre-calibrated NiTi closed coil springs with a relatively constant force delivery (American Orthodontics India Private Ltd, Bengaluru, Karnataka, India), placed bilaterally from the mini-implants to the crimpable hooks placed between the lateral incisor and canine on each side (Figure 1). The patient was reviewed periodically, once every 3 weeks for 6 months.

Figure 1. Distalizing force applied with NiTi closed coil springs placed bilaterally from the attachments placed between the maxillary incisor and canine to miniimplants inserted between the maxillary second premolar and the first permanent molar.
OIIRR was assessed with CBCT taken prior to the start of distal movement (T1) and six months after distal movement (T2). All CBCTs were obtained with the same machine, the Sidexis XG 2.63 machine (2016 Sirona Dental Systems, GmbH), with the following specifications: 90 kV, 9-12 mA, 8-14-second exposure time, 200 microns voxel resolution, and 80 X 80 mm field of view (FOV).
The DICOM (Digital Imaging and Communications in Medicine) images were viewed using a Galileos viewer 1.9. The DICOM data was reconstructed at 0.125 mm increments. All the teeth from the second molar on the right side to the second molar on the left side were checked for the presence of OIIRR.
The slicing window was placed on the tooth for measurement in the panoramic view. The DICOM image in the axial view of the panoramic window was adjusted so that the cross-hair was at the apex of the root. The cross-sectional and tangential views were adjusted so that the entire length of the tooth was visible. The change in the tooth apex was evaluated for blunting16 at T1 and T2 (Figures (2 and (3). The presence of blunting confirmed OIIRR. The apex of each tooth from the maxillary central incisor to the maxillary second molar was examined individually on each side of the maxillary arch for the presence or absence of OIIRR and tabulated. The presence of blunting in any of the roots of a multi-rooted tooth was considered as the presence of OIIRR.

Figure 2. Root apex of the maxillary left lateral incisor prior to the start of distalization of the entire maxillary teeth (T1). Note the curve of the apex without blunting of the root apex, indicating the absence of OIIRR.

Figure 3. Root apex of the same maxillary left lateral incisor six months after distal movement of the entire maxillary teeth (T2). Note the blunting of the root apex, indicating the presence of OIIRR.
The CBCT was assessed by an expert with more than 15 years of experience in orthodontics and more than 20 years of experience in dentistry. Twenty-eight teeth were reassessed to check for intraoperator reliability.
Descriptive statistics with frequency distribution and percentage of OIIRR were evaluated on all the teeth from the maxillary second permanent molar to the maxillary permanente central incisor on both sides. Intraoperator reliability was checked using the intraclass correlation coefficient.
Results
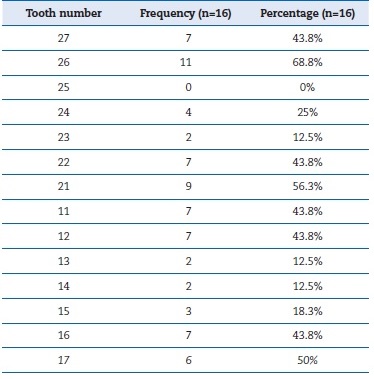
The patients’ mean age was 17.13 ± 7.81 years. The intraclass correlation coefficient was 0.82, indicating good reliability. OIIRR was present in almost all the teeth, except the left second premolar. The prevalence of OIIRR was greater in molars and incisors and least in the premolars. The percentage of distribution was highest in the right maxillary first permanente molar (68.8%), followed in descending order by the right maxillary central incisor (56.3%), the left and right maxillary second permanent molars (50% and 43.8%), the maxillary right central and lateral incisors and the maxillary left permanente second molar (43.8%), the maxillary left first premolar (25%), the maxillary right second premolar (18.3%), and the maxillary first premolar and the canines of both sides (12.5%). Only the maxillary left second premolar did not show the presence of OIIRR (0%) (Table 1). In the molars, the prevalence of OIIRR was highest in the distobuccal root, followed by the mesiobuccal root and the palatal root.
Table 1. Prevalence of orthodontically induced inflammatory root resorption in all the teeth of the maxillary arch as a result of distal movement of the maxillary teeth with mini-implants.
Discussion
There are various types of root resorption that can result in tooth damage. It may occur due to OIIRR, pre-eruptive intracoronal resorption, or root resorption due to apical periodontitis.
Apical root resorption due to pulpitis is the most prevalent form of root resorption. Pre-eruptive intracoronal resorption may also damage the tooth and occurs frequently in the upper canines and lower premolars.17 OIIRR is na undesirable complication of orthodontic treatment. The presence of OIIRR is very common and has been frequently reported in the literature. Prompt identification is of paramount importance to avoid harmful effects on the tooth.
Until recently, conventional radiographs were used to assess the incidence of OIIRR. Since radiographs represente the two-dimensional projection of a three-dimensional object, resorption may be masked by the overlap of adjacente structures. Use of a three-dimensional imaging system, such as the CBCT, may be advantageous in these situations. Thus, the use of cone-beam computed tomography to evaluate OIIRR is more likely to yield accurate results than conventional radiographic methods.18 CBCT has several applications in orthodontics,19 - 22 such as impacted tooth localization, OIIRR, fractured roots, orthodontic implant placement, location of anatomic structures, asymmetry evaluation, temporomandibular joint assessment, cleft lip and palate, conebeam computed tomography-generated cephalograms, airway analysis, jaw pathologies, orthognathic surgery, and superimpositions.
Several factors must be considered while assessing OIIRR, including age, sex, root form, treatment duration, dimension of the arch wire, use of torquing auxiliaries, uprighting springs, and Class II elastics.23, 24 The presence of third molars, buccally or lingually tipped molars, premolar and anterior teeth touching the cortical plate, and the shape of the roots may be associated with OIIRR.
The incidence of OIIRR increases with age2 due to decreased vascularity of the periodontal membrane and increased bone density. However, in this study, the sample consisted of only young individuals. Earlier studies showed that the incidence of OIIRR is higher in anterior teeth25 compared to posterior teeth, and more common in the maxillary arch compared to the mandibular arch during conventional orthodontic treatment.26 In the current study, where all the maxillary teeth were moved with orthodontic forces applied from mini-implants, comparison of OIIRR between the anterior and posterior teeth revealed a greater percentage of OIIRR on the posterior teeth. In conventional retraction mechanics, the maxillary molar teeth act as the anchorage unit and do not move effectively with applied force compared to the distal movement of all the maxillary teeth. This may explain the lower incidence of OIIRR in the posterior teeth with conventional mechanics.
Since the duration of orthodontic treatment affects the severity of OIIRR, all patients in the current study were evaluated over a six-month period. Despite the short treatment
duration, OIIRR was noted in most teeth. Earlier studies have shown that the severity of OIIRR was greater when mini-implants were used as anchorage compared to conventional retraction mechanics with the posterior teeth as anchorage.27, 28 Every different type of orthodontic tooth movement is associated with a variable degree of OIIRR. Studies reported in the literature reveal that molar intrusion performed with mini-implants produced a clinically significant degree of intrusion with little or no resorption.29 However, distal movement of the maxillary teeth evaluated in the present study was associated with OIIRR in several teeth. OIIRR may also occur due to contact of the root of the tooth with the mini-implant. However, this resorption is repaired unless the pulp is injured.30 The effect of low-intensity pulsed ultrasound may reduce the effect of OIIRR and is being evaluated.31, 32
The use of CBCT is associated with radiation exposure. CBCT has lower radiation exposure than CT when used for orthodontic diagnosis, treatment planning, and evaluation of growth and treatment effects.33 However, the amount of radiation exposure from a CBCT is greater than that associated with an orthopantomogram. A reduction in the CBCT machine’s FOV, along with appropriate scanning protocols and shielding devices, such as a thyroid collar and eyeglasses, may help reduce radiation exposure. Reducing the size of the FOV reduces the patient’s exposure to ionizing radiation, reduces scatter, improves the resolution of the image, and has the same level of performance as CBCT with a large FOV.34 35 However, there is conflicting evidence regarding the level of radiation exposure with CBCT with a small FOV compared with conventional radiographs taken for orthodontic purposes, with one study stating that CBCT protocols such as shielded low-dose CBCT have a lower effective dose than conventional panoramic and lateral cephalometric radiographs,35 while others refute these results.36 Either way, care should be taken when CBCT images are obtained for pediatric patients, as the absorbed dose may be higher in children than in adults.36 If CBCT is required in pediatric patients, the effective dose has to be minimized and optimized, as they are more susceptible to the harmful effects of radiation than adults.37
Some of the applications of CBCT, especially with a small FOV, in orthodontics, beyond OIIRR assessment, include periodontal evaluation, mini-implant placement, evaluation of alveolar or basal bone defects, and localization of impacted teeth. Other CBCT applications in dentistry include its use in endodontics to study the anatomy of difficult root canal systems and extra canals after treatment failure, missed or extra canals, perforations, broken instruments, chronic periapical periodontitis, root fracture, and dental trauma.38 A CBCT taken for any of the above conditions may be used to assess OIIRR.
CBCT should not be recommended for routine use in orthodontic patients as a substitute for a conventional set of radiographs.37 Appropriate imaging protocols, such as reducing the FOV and shielding sensitive organs, are advisable methods and must be implemented to lower the exposure dose.
This preliminary study establishes the presence of OIIRR during distal movement of the maxillary teeth with mini-implants. It did not evaluate the influence of sex, age, presence of third molars, root apex shape, and bone density on the severity of OIIRR and on the prevalence of OIIRR in individual roots of multi-rooted teeth, so further studies should be conducted to evaluate these factors.
The measurements made in this study can be performed in subjects in another clinical setting following the procedure described in the present study.
Conclusions
The incidence of OIIRR during the distal movement of the maxillary teeth was very high. The percentage of OIIRR was greater in the posterior teeth compared to the anterior teeth and was very low in the premolar region. Care must be taken to avoid tooth damage due to OIIRR during distal movement of the maxillary teeth using mini-implants as anchorage.
References
1. Lopatiene K, Dumbravaite A. Risk factors of root resorption after orthodontic treatment. Stomatologija. 2008;10:89-95.
2. Dindaroğlu F, Doğan S. Root Resorption in Orthodontics. Turk J Orthod. 2016;29:103-8.
3. Mirabella AD, Artun J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108:48-55.
4. Chang CH, Lin JS, Roberts WE. Failure rates for stainless steel versus titanium alloy infrazygomatic crest bone screws: A single-center, randomized double-blind clinical trial. Angle Orthod. 2019;89:40-6.
5. Bechtold TE, Kim JW, Choi TH, Park YC, Lee KJ. Distalization pattern of the maxillary arch depending on the number of orthodontic miniscrews. Angle Orthod. 2013;83:266-73.
6. Park HS, Lee SK, Kwon OW. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod. 2005;75:602-9.
7. Yamada K, Kuroda S, Deguchi T, Takano-Yamamoto T, Yamashiro T. Distal movement of maxillary molars using miniscrew anchorage in the buccal interradicular region. Angle Orthod. 2009;79:78-84.
8. Felicita AS, Thomas LA. Overall treatment outcome achieved during distal movement of the entire maxillary dentition using mini-implants–A single-center analytical observational clinical study. Rev Port Estomatol Med Dent Cir Maxilofac. 2022;63:3-11.
9. Sa’aed NL, Park CO, Bayome M, Park JH, Kim Y, Kook YA. Skeletal and dental effects of molar distalization using a modified palatal anchorage plate in adolescents. Angle Orthod. 2015;85:657-64.
10. Lee SK, Abbas NH, Bayome M, Baik UB, Kook YA, Hong M, et al. A comparison of treatment effects of total arch distalization using modified C-palatal plate vs buccal miniscrews. Angle Orthod. 2018;88:45-51.
11. Maki K, Inou N, Takanishi A, Miller AJ. Computer-assisted simulations in orthodontic diagnosis and the application of a new cone beam X-ray computed tomography. Orthod Craniofac Res. 2003;6(Suppl1):95-182.
12. Lagravère MO, Carey J, Toogood RW, Major PW. Threedimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2008;134:112-6.
13. Li Y, Deng S, Mei L, Li Z, Zhang X, Yang C, et al. Prevalence and severity of apical root resorption during orthodontictreatment with clear aligners and fixed appliances: a cone beam computed tomography study. Prog Orthod. 2020;21:1.
14. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6:14-7.
15. Felicita AS. A simple three-dimensional stent for proper placement of mini-implant. Prog Orthod. 2013;14:45.
16. Sharpe W, Reed B, Subtelny JD, Polson A. Orthodontic relapse, apical root resorption, and crestal alveolar bone levels. Am J Orthod Dentofacial Orthop. 1987;91:252-8.
17. Gurunathan D, Pandiar D, Krishnan RP. Global prevalence of pre eruptive intracoronal resorption (PEIR) of teeth: a systematic review of literature. Eur Arch Paediatr Dent. 2025;26:225-32.
18. Sherrard JF, Rossouw PE, Benson BW, Carrillo R, Buschang PH. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137:S100-8.
19. Kau CH, Richmond S, Palomo JM, Hans MG. Threedimensional cone beam computerized tomography in orthodontics. J Orthod. 2005;32:282-93.
20. Kapila SD, Nervina JM. CBCT in orthodontics: assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol. 2015;44:20140282.
21. Agrawal JM, Agrawal MS, Nanjannawar LG, Parushetti AD. CBCT in orthodontics: the wave of future. J Contemp Dent Pract. 2013;14:153-7.
22. Coşkun İ, Kaya B. Cone Beam Computed Tomography in Orthodontics. Turk J Orthod. 2018;31:55-61.
23. Levander E, Malmgren O. Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988;10:30-8.
24. Noori RM, Ahmed OK, Kadhum AS, Yassir YA, Di Blasio M, Russo D, et al. The Effectiveness of Conventional and Advanced Aligning Archwires: The Insights of Two Randomized Clinical Trials. Eur J Dent. 2025;19:985-97.
25. Blake M, Woodside DG, Pharoah MJ. A radiographic comparison of apical root resorption after orthodontic treatment with the edgewise and Speed appliances. Am J Orthod Dentofacial Orthop. 1995;108:76-84.
26. Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119:505-10.
27. Barros SE, Janson G, Chiqueto K, Baldo VO, Baldo TO. Root resorption of maxillary incisors retracted with and without skeletal anchorage. Am J Orthod Dentofacial Orthop. 2017;151:397-406.
28. Lund H, Gröndahl K, Hansen K, Gröndahl HG. Apical root resorption during orthodontic treatment. A prospective study using cone beam CT. Angle Orthod. 2012;82:480-7.
29. Carrillo R, Rossouw PE, Franco PF, Opperman LA, Buschang PH. Intrusion of multiradicular teeth and related root resorption with mini-screw implant anchorage: a radiographic evaluation. Am J Orthod Dentofacial Orthop. 2007;132:647-55.
30. Alves M Jr, Baratieri C, Mattos CT, Araújo MT, Maia LC. Root repair after contact with mini-implants: systematic review of the literature. Eur J Orthod. 2013;35:491-9.
31. Vaddamanu SK, Alhamoudi FH, Vyas R, Gurumurthy V, Siurkel Y, Cicciù M, et al. Attenuation of orthodontically induced inflammatory root resorption by using low-intensity pulsed ultrasound as a therapeutic modality- a systematic review. BMC Oral Health. 2024;24:67.
32. Alqahtani AA, Alam MK, Alahmari BS, Srivastava KC. Effects of low-level laser therapy on orthodontic tooth movement: Evaluation of bone density changes via 3DCBCT. Bangladesh Journal of Medical Science. 2025;24:133–43.
33. Grauer D, Cevidanes LS, Proffit WR. Working with DICOM craniofacial images. Am J Orthod Dentofacial Orthop. 2009;136:460-70.
34. Dillenseger JP, Gros CI, Sayeh A, Rasamimanana J, Lawniczak F, Leminor JM, et al. Image quality evaluation of small FOV and large FOV CBCT devices for oral and maxillofacial radiology. Dentomaxillofac Radiol. 2017;46:20160285.
35. Ting S, Attaia D, Johnson KB, Kossa SS, Friedland B, Allareddy V, et al. Can modifying shielding, field of view, and exposure settings make the effective dose of a cone-beam computed tomography comparable to traditional radiographs used for orthodontic diagnosis? Angle Orthod. 2020;90:655-64.
36. Signorelli L, Patcas R, Peltomäki T, Schätzle M. Radiation dose of cone-beam computed tomography compared to conventional radiographs in orthodontics. J Orofac Orthop. 2016;77:9-15.
37. Choi E, Ford NL. Measuring absorbed dose for i-CAT CBCT examinations in child, adolescent and adult phantoms. Dentomaxillofac Radiol. 2015;44:20150018.
38. Kaur K, Saini RS, Vaddamanu SK, Bavabeedu SS, Gurumurthy V, Sainudeen S, et al. Exploring Technological Progress in Three-Dimensional Imaging for Root Canal Treatments: A Systematic Review. Int Dent J. 2025;75:1097-112.
A. Sumathi Felicita
E-mail address: sumifeli@hotmail.com
CRediT authorship contribution statement
A. Sumathi Felicita: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Writing – original draft, Writing – review & editing. T.N. Uma Maheswari: Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
1646-2890/© 2025 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).