
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2025 | 66 (4) | 207-212
Clinical case
Multiple intraoral salivary duct cysts: Report of a rare case
Múltiplos cistos do ducto salivar intraoral: Relato de um caso raro
a Department of Bioscience and Oral Diagnosis, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
b Department of Dental Materials and Prosthodontics, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
c Department of Surgery and Diagnosis, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
Luis Augusto de Almeida-Silva - luis.almeida-silva@unesp.br
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 66
Issue - 4
Clinical case
Pages - 207-212
Go to Volume
Article History
Received on 30/01/2025
Accepted on 30/11/2025
Available Online on 22/12/2025
Keywords
Clinical Case Report
Multiple intraoral salivary duct cysts: Report of a rare case
Múltiplos cistos do ducto salivar intraoral: Relato de um caso raro
Luis Augusto de Almeida-Silva1,* 0000-0001-8668-595X
Brunna da Silva Nobrega Souza1 0000-0003-1735-8220
Juliana dos Santos Lupp1 0000-0003-0621-4774
Leonardo Alvares Sobral-Silva2 0000-0002-6743-4423
Michelle Bianchi-de-Moraes3 0000-0002-7945-2098
1 Department of Bioscience and Oral Diagnosis, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
2 Department of Dental Materials and Prosthodontics, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
3 Department of Surgery and Diagnosis, Institute of Science and Technology, São Paulo State University (Unesp), São José dos Campos, Brazil
Article history:
Received 30 January 2025
Accepted 30 November 2025
Available online 19 December 2025
Abstract
The salivary duct cyst predominantly presents as a single lesion in the major salivar glands. The occurrence of multiple lesions in minor salivary glands is extremely rare, with only three cases reported in the literature. This case report presents a new case of multiple salivary duct cysts in minor salivary glands. A 62-year-old woman sought dental care, complaining of the sudden appearance of a painful nodule on the upper lip. Intraoral examination revealed multiple submucosal nodules, mobile and slightly tender, occasionally draining mucus through dilated openings, located on the labial and buccal mucosa. Based on the clinical hypotheses of salivary duct cyst, cystadenoma, and canalicular adenoma, an excisional biopsy of the referred nodule was performed under local anaesthesia. Microscopic analysis revealed multiple cystic lesions lined with epithelium that was either cuboidal, squamous, or pseudostratified columnar, with a lumen filled with mucous material. By correlating these findings with the clinical characteristics, the final diagnosis of multiple intraoral salivary duct cysts was established. The analysis of this and other cases broadens the understanding of the etiopathogenic factors involved and aids the recognition of multiple salivary duct cyst lesions in minor salivary glands in clinical and laboratory practice.
Keywords: Case reports, Cysts, Minor salivary gland, Salivary ducts
Resumo
O cisto do ducto salivar apresenta-se predominantemente como uma única lesão nas glândulas salivares maiores. A ocorrência de múltiplas lesões nas glândulas salivares menores é extremamente rara, com apenas três casos relatados na literatura. Este relato de caso apresenta um novo caso de múltiplos cistos do ducto salivar em glândulas salivares menores. Uma mulher de 62 anos procurou atendimento com queixa de aparecimento súbito de um nódulo doloroso no lábio superior. O exame intraoral revelou múltiplos nódulos submucosos, móveis e ligeiramente dolorosos, que ocasionalmente drenavam muco através de aberturas dilatadas, localizados nas mucosas labial e bucal. Com base nas hipóteses clínicas de cisto do ducto salivar, cistadenoma e adenoma canalicular, foi realizada uma biópsia excisional do nódulo referido sob anestesia local. A análise microscópica revelou múltiplas lesões císticas revestidas por epitélio cuboide, escamoso ou colunar pseudostratificado, com lúmen preenchido por material mucoso. Através da correlação destes achados com as características clínicas, o diagnóstico final de múltiplos cistos do ducto salivar intraoral foi estabelecido. A análise deste e de outros casos amplia a compreensão dos fatores etiopatogénicos envolvidos e auxilia no reconhecimento das lesões múltiplas do cisto do ducto salivar em glândulas salivares menores na prática clínica e laboratorial.
Palavras-chave: Relatos de caso, Cistos, Glândula salivar menor, Ductos salivares
Introduction
Salivary duct cyst (SDC), also known as sialocyst, is a condition that typically affects the major salivary glands and is characterized by salivary duct dilation secondary to obstruction.
Although rare, SDC can also occur in the minor salivar glands (MSGs), where it is referred to as “intraoral salivar duct cyst”.1 In such cases, the lesion presents as a single nodule, often asymptomatic, which may be firm or fluctuant upon palpation, with a coloration ranging from pink to bluish and measuring between 3 and 15 mm in diameter. This condition can occur in any region with MSGs but is more commonly found on the floor of the mouth, the labial mucosa, and the buccal mucosa, particularly in women in their sixth decade of life.1 – 3
The occurrence of multiple lesions is even rarer than the isolated involvement of MSGs2 and poses a diagnostic challenge as it may be mistaken for other conditions that exhibit this clinical pattern more frequently. In this context, we report a new case of multiple intraoral salivary duct cysts (MISDCs) accompanied by a review of the literature to contextualize their characteristics with those of other reported cases and to expand knowledge of this atypical presentation.
Case report
A 62-year-old Caucasian woman sought dental care complaining of the sudden growth of a “lump on the upper lip” accompanied by pain, which had appeared four weeks before the consultation. During the anamnesis, she reported a medical history of hypertension, left mitral valve hypertrophy, and hyperlipidemia, using acetylsalicylic acid, simvastatin, valsartan, and atenolol for disease control. The patient also mentioned that, shortly before the consultation, the lesion had discharged a thick yellowish exudate. Concerned about the progression of her condition, she self-medicated with azithromycin 500 mg, taking one tablet daily for three days. In addition to the aforementioned lesion (Figure 1), the intraoral examination revealed multiple submucosal nodules with a color similar to the adjacent mucosa and approximately 9.0 mm in diameter that were mobile, slightly painful, firm to palpation, and diffusely distributed across the upper and lower labial mucosa, as well as the buccal mucosa. Some displayed dilated openings that discharged mucus upon pressing (Figures 2,3, 4, and 5).

Figure 1. Clinical aspect of the lesion that prompted the complaint. A marked dilation of the ductal orifice is observed, with slight protrusion of the adjacente mucosa.

Figure 2. Clinical aspect of the nodules distributed on the right side of the upper lip.

Figure 3. Clinical aspect of the nodules distributed on the left buccal mucosa.

Figure 4. Clinical aspect of the nodules distributed on the right side of the lower lip. Discrete points of ductal dilation are observed in some of the nodules.

Figure 5. Clinical aspect of the nodules distributed on the left side of the lower lip. Discrete points of d
Based on these findings, the clinical diagnostic hypotheses considered were: SDC, cystadenoma of the salivary glands, and canalicular adenoma.
For confirmation, an excisional biopsy of the initially referred nodule was performed under local anesthesia with mepivacaine hydrochloride 2% (20 mg/mL) + epinephrine 1:100.000 (μg/mL), and the specimen was sent to the oral and maxillofacial pathology laboratory. Microscopic examination of histological sections revealed cystic lesions lined by cuboidal, columnar, or squamous epithelium with two to three cellular layers, sometimes displaying ciliated cells, with áreas of apocrine and mucous metaplasia. The lumen contained mucous material mixed with some inflammatory and desquamated epithelial cells. The lesions were associated with lobules of MSGs exhibiting multiple significantly dilated ducts (Figures 6, 7, and 8). Based on the clinicopathological correlation features, the final diagnosis of MISDC was established.
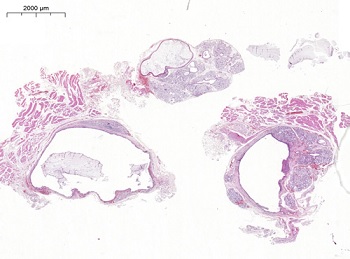
Figure 6. Histopathological aspects of the multiple cystic lesions associated with lobules of MSGs (hematoxylin and eosin stain, 2X original magnification).
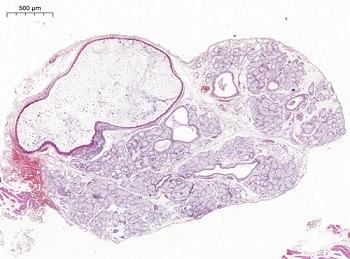
Figure 7. MSG showing a cystically dilated interlobular duct and significantly dilated intralobular ducts. A variable amount of mucus is present in the lumen (hematoxylin and eosin stain, 5X original magnification).
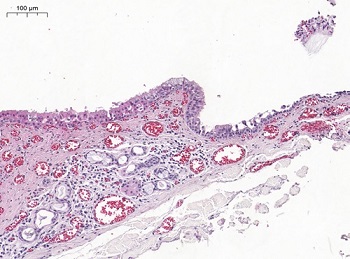
Figure 8. Cystic lining epithelium with a gradual transition in thickness, showing, in the thicker portion, epithelial cells with apocrine metaplasia, pseudostratified columnar cells with mucus and cilia, and cells with mucous metaplasia; and in the thinner portion, columnar, cuboidal, and squamous cells (hematoxylin and eosin stain, 20X original magnification).
At the six-month follow-up, the lesion that prompted the patient’s complaint was fully healed (Figure 9). The remaining lesions identified during the clinical examination demonstrated no evidence of progression or significant alteration, and no new lesions had developed.

Figure 9. Clinical aspect of the lesion site six months after excisional biopsy, showing complete healing and absence of recurrence.
Discussion and conclusions
Given the rarity of MISDC cases, we conducted an extensive literature review in search of clinical reports on this condition. By December 2024, strategies were implemented, and searches were performed in the PubMed, Scopus, and Google Scholar databases, as well as in the reference lists of articles, without restrictions on language or publication date, and including only fully published documents. To date, the literature has only three cases of MISDC: two reported by Tal et al.4 and one by Jahanshahi et al.5
The etiopathogenesis of this condition remains uncertain, but it is suggested that local and/or systemic factors may compromisse the homeostasis of MSGs and alter saliva properties, thereby promoting total or partial ductal obstruction. The obstruction caused by mucus secretion stasis may range from na intraluminal focus to a mucus plug, leading to increased pressure and ductal dilation.2–5 Tal et al.4 postulate that their cases were caused by the patients’ advanced age, comorbidities, and medication use, while Jahanshahi et al.5 attributed such changes to smoking. These factors were also observed in the present case (Table 1).
Table 1. Factors associated with the reported cases (including the present case)
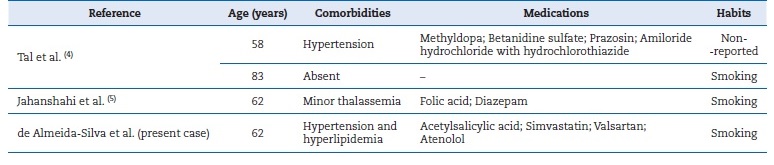
Aging is accompanied by a progressive decline in physiological functions.6 Accordingly, MSGs are affected by aging, exhibiting acinar atrophy, fibrosis,6, 7 and replacement of parenchyma with adipose tissue.7 Chronic diseases and medication use also increase with age.8 In the present case and in one of Tal et al.’s cases,4 the patients used antihypertensive and ß-blocker medication. Hypertensive patients exhibit more viscous saliva with a lower pH even before using antihypertensive drugs,8, 9 which are associated with inducing glandular dysfunction10 and reducing the salivary secretion rate,4 thus favoring mucus stasis and ductal obstruction.4, 8, 9
Smoking acts synergistically, promoting alterations in saliva properties and damage to MSGs. The short ducts of these glands open into the oral mucosa and, because their openings are non-keratinized, they become vulnerable to external injuries, allowing tobacco products to enter and cause inflammation around the openings.11 These inflammations affect both the ducts and the parenchyma of MSGs. Studying the effects of tobacco on MSGs in the hard palate, Eliasson et al.11 observed ductal dilation with mucus retention, inflammatory cell accumulation in the stroma, and acinar atrophy. Furthermore, they suggested that tobacco’s vasoconstrictive effects could compromise long-term salivary secretion due to its dependence on the blood supply. Such changes affect salivary flow and composition,11 and may influence ductal obstruction and the formation of multiple cysts.
The lesions in our case exhibited clinical characteristics similar to those described in the previous reports, presenting as sessile nodules, firm to palpation, with coloration resembling the adjacent mucosa, sometimes with dilated openings discharging mucus, located on the buccal and labial mucosa of elderly individuals.
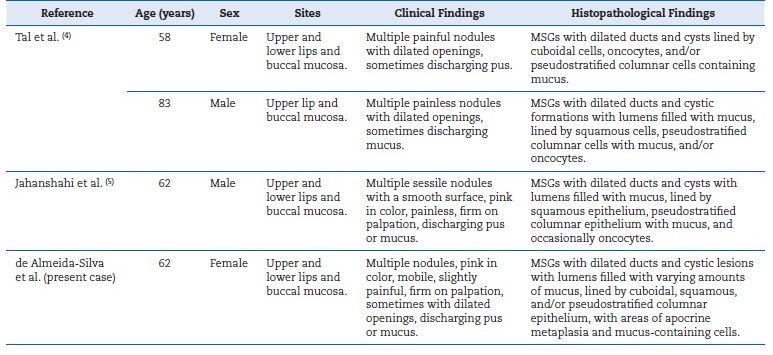
Although pain is uncommon, sensitivity may occur and become intense with MSGs infections,4 as seen here and in one of Tal et al.’s cases4 (Table 2). Individually, these aspects do not differ significantly from the clinical presentation of single SDC lesions.2, 4, 5 However, the unusual occurrence of multiple nodules with mucus discharge and widespread distribution across the labial and buccal mucosa may complicate identification when compared to other lesions with similar characteristics.
Table 2. Clinical and histopathological characteristics of the reported cases (including the present case)
Among these lesions, we considered canalicular adenoma and cystadenoma of the salivary gland as differential diagnoses, in contrast to the reviewed cases,4, 5 which included glandular cheilitis. We did not consider glandular cheilitis due to its typical presentation of reddened ductal ostia, swelling, and crust formation on the lips —features divergent from those in the present case, as well as the rarity of lesions on the buccal mucosa.12 Canalicular adenoma and salivary gland cystadenoma, however, may clinically mimic MISDC, as both can presente as multifocal nodules with coloration resembling the adjacente mucosa that are firm or slightly fluctuant on palpation, commonly located on the labial and buccal mucosae, and primarily found in older women13 – 15.
Another important differential diagnosis to consider is mucocele (mucus extravasation phenomenon). Although frequently presenting on MSGs of the lower labial mucosa as a solitary lesion,2 mucoceles can, in rare instances, appear on the upper labial mucosa16 or as multiple lesions.17 In such cases, their clinical appearance, such as mobile soft nodules that can discharge mucus upon pressing,2, 16, 17 may closely resemble those of MISDC.
Given the clinical similarities among these differential diagnoses, analysis of histopathological characteristics is essential for distinguishing among the entities. As in the present case, all reported cases of MISDC revealed cystically dilated ducts lined by cuboidal, squamous, and/or pseudostratified columnar epithelium containing mucus, in addition to a lumen filled with mucous material (Table 2). In contrast, a mucocele presents as a cavity lined by granulation tissue, rather than epithelial tissue, a key histological difference that distinguishes it from MISDC.1, 2, 16 In turn, canalicular adenoma is characterized by the proliferation of narrow and elongated ductal structures that connect in networks,13, 14 a pattern absent in MISDC. On the other hand, cystadenomas of the salivary glands may show similar dilated ducts but differ from MISDC by the absence of a capsule and the presence of an adenomatous component and papillary projections with a fibrovascular nucleus.1, 15
Therefore, the analysis of this case together with the reviewed cases indicates that factors such as aging, chronic diseases, medications, and smoking influence the pathogenesis of MISDC. Although the clinicopathological characteristics do not differ significantly from those of single cysts, the rare occurrence of multiple lesions in MSGs poses a diagnostic challenge.
This study expands the understanding of this rare condition, providing important insights for clinical recognition and an additional basis for investigations into the interactions between systemic conditions and alterations in MSG properties.
References
1. Stojanov IJ, Malik UA, Woo S Bin. Intraoral salivary suct cyst: clinical and histopathologic features of 177 cases. Head Neck Pathol. 2017;11:469–76.
2. Brooks JK, Funari GJ, Basile JR. Salivary gland duct cyst arising in a minor salivary gland on the floor of the mouth: A case report. Quintessence Int. 2017;48:325–8.
3. Eversole LR. Oral sialocysts. Arch Otolaryngol Head Neck Surg.1987;113:51-6.
4. Tal H, Altini M, Lemmer J. Multiple mucous retention cysts of the oral mucosa. Oral Surg Oral Med Oral Pathol. 1984;58:692-5.
5. Jahanshahi G, Shirani A, Khozeimeh F. Multiple Mucous Retention Cysts (Mucocele) of the Oral Mucosa : A Case Report. Dent
6. Vissink A, Spijkervet FK, Amerongen AVN. Aging and saliva: a review of the literature. Spec Care Dentist. 1996;16:95-103.
7Klein A, Klein J, Chacham M, Kleinman S, Shuster A, Peleg O, et al. Acinar Atrophy, Fibrosis and Fatty Changes Are Significantly More Common than Sjogren’s Syndrome in Minor Salivary Gland Biopsies. Medicina (Kaunas). 2022;58:175.
8. Kagawa R, Ikebe K, Enoki K, Murai S, Okada T, Matsuda K, et al. Influence of hypertension on pH of saliva in older adults. Oral Dis. 2013;19:525-9.
9. Mohiti A, Eslami F, Dehestani MR. Does Hypertension affect Saliva Properties? J Dent (Shiraz). 2020;21:190-4.
10. Wolff A, Joshi RK, Ekström J, Aframian D, Pedersen AM, Proctor G, et al. A Guide to Medications Inducing Salivary Gland Dysfunction, Xerostomia, and Subjective Sialorrhea: A Systematic Review Sponsored by the World Workshop on Oral Medicine VI. Drugs R D. 2017;17:1-28.
11. Eliasson L, Heyden G, Landahl S, Steen B. Effects of tobacco and diuretics on human palatal salivary glands. J Oral Pathol Med. 1991;20:126-9.
12. Nico MMS, Nakano de Melo J, Lourenço SV. Cheilitis glandularis: A clinicopathological study in 22 patients. J Am Acad Dermatol. 2010;62:233–8.
13. Rousseau A, Mock D, Dover DG, Jordan RC. Multiple canalicular adenomas: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:346-50.
14. Thompson LD, Bauer JL, Chiosea S, McHugh JB, Seethala RR, Miettinen M, et al. Canalicular adenoma: a clinicopathologic and immunohistochemical analysis of 67 cases with a review of the literature. Head Neck Pathol. 2015;9:181-95.
15. Tjioe KC, de Lima HG, Thompson LD, Lara VS, Damante JH, de Oliveira-Santos C. Papillary Cystadenoma of Minor Salivary Glands: Report of 11 Cases and Review of the English Literature. Head Neck Pathol. 2015;9:354-9.
16. Mustapha IZ, Boucree SA Jr. Mucocele of the upper lip: case report of an uncommon presentation and its differential diagnosis. J Can Dent Assoc. 2004;70:318-21. https://www.cdaadc.ca/jadc/vol-70/issue-5/318.html
17. Xu GZ, Yang C, Yu CQ, He D, Zhang S. Multiple superficial mucoceles on lower lip, soft palate, retromolar region, and floor of mouth. J Oral Maxillofac Surg. 2010;68:2601-3.
Luis Augusto de Almeida-Silva
E-mail address: luis.almeida-silva@unesp.br
CRediT authorship contribution statement
Luis Augusto de Almeida-Silva: Conceptualization, Data curation, Formal analysis, Investigation, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. Brunna da Silva Nobrega Souza: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. Juliana dos Santos Lupp: Investigation, Writing – original draft, Writing – review & editing. Leonardo Alvares Sobral‑Silva: Investigation, Writing – original draft, Writing – review & editing. Michelle Bianchi-de-Moraes: Conceptualization, Formal analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
1646-2890/© 2025 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).