
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
Rev Port Estomatol Med Dent Cir Maxilofac | 2017 | 58 (1) | 39-45
Original research
Biomechanical study of dentists posture when using a conventional chair versus a saddle-seat chair
Estudo biomecânico da postura do médico dentista utilizando um banco convencional versus banco em sela
a Faculty of Engineering, University of Porto, Porto, Portugal.
b Porto Biomechanics Laboratory, Porto, Portugal.
c Faculty of Dental Medicine, University of Porto, Porto, Portugal.
Vanessa Silva - vanessa.m.b.ss@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 58
Issue - 1
Original research
Pages - 39-45
Go to Volume
Article History
Received on 11/08/2016
Accepted on 08/12/2016
Available Online on 31/03/2017
Keywords
Original research
Biomechanical study of dentists’ posture when using a conventional chair versus a saddle-seat chair
Estudo biomecânico da postura do médico dentista utilizando um banco convencional versus banco em sela
Vanessa Silvaa,*, Pedro Fonsecab, Maria Eugénia Pinhoa, Joaquim Góisa, Mário Vaza, José Reis-Camposc
a Faculty of Engineering, University of Porto, Porto, Portugal.
b Porto Biomechanics Laboratory, Porto, Portugal.
c Faculty of Dental Medicine, University of Porto, Porto, Portugal.
http://doi.org/10.24873/j.rpemd.2017.05.005
Abstract
Objectives: This study aimed to provide information about dentists’ body posture on a conventional chair vs. a saddle-seat chair while performing dental procedures. Information was obtained using inertial motion sensors.
Methods: Twenty-four dentists performed a Class I cavity in the upper right and left first molars and lower right and left first molars. Nineteen dentists worked on a conventional chair (Group I), and five on a saddle-seat chair (Group II). Kinematic measurements of the whole body were registered using Xsens® MVN BIOMECH.
>Results: Both groups worked with a pronounced forward head position. Lateral flexion of the head was similar between groups, and head rotation was more evident in Group II. Regarding trunk position, Group II showed less forward leaning and lateral flexion than Group I. Arm elevation of both the left and right arms was more pronounced in Group I during all dental tasks. However, Group I showed better left-hand posture. Anterior rotation of the pelvis was most evident while working on the lower jaw in Group II.
Conclusions: This study suggests that the saddle seat improves the working posture regarding pelvis rotation, arm elevation, and trunk flexion. Further studies should include objective measurements of the dentists’ posture during dental work using different dental equipment, to understand the role of ergonomics in dentistry.
Keywords: Dentist, Ergonomics, Posture
Resumo
Objetivos: O objetivo deste estudo é obter informação postural dos segmentos corporais do médico dentista, enquanto trabalha numa cadeira convencional vs cadeira ergonómica, através de sensores de movimento.
Métodos: Vinte e quatro dentistas realizaram uma cavidade tipo I (oclusal) no primeiro molar de cada quadrante dentário. Dezanove dentistas trabalharam numa cadeira convencional (Grupo I) e cinco dentistas numa cadeira ergonómica (Grupo II). Com recurso aos sensores Xsens® MVN BIOMECH registou-se as posições de cada participante.
Resultados: Os dois grupos trabalharam com excessiva flexão anterior da cabeça. A flexão lateral foi similar entre grupos e a rotação foi mais evidente no Grupo II. O Grupo II apresentou menores valores de flexão anterior e lateral do tronco. No Grupo I a elevação de ambos os braços foi mais evidente durante todas as tarefas. No entanto o Grupo I apresentou melhor postura da mão esquerda comparada com o Grupo II. Rotação anterior da pélvis foi mais evidente no Grupo II durante o trabalho no maxilar inferior.
Conclusões: Este estudo sugere que o banco em sela melhora a postura do médico dentista no que diz respeito à rotação da pélvis, elevação dos braços e flexão do tronco. Investigações futuras devem incluir medidas objetivas da postura do dentista durante a atividade clínica com recurso a diferentes equipamentos dentários, no sentido de compreender o papel da ergonomia na medicina dentária.
Palavras-chave: Dentista, Ergonomia, Postura
Introduction
The dental profession is considered a high‑risk job for musculoskeletal disorders, as dentists frequently adopt awkward body postures that can have serious consequences on their health.1 ,2The standing and sitting postures and the bending and rotation of the trunk may cause these disorders when there is an excessive strain or compression of the tissues.3‑ 7
Different authors have shown that, during clinical activity, dentists bend their head anteriorly and laterally repetitively over long periods. This combination of movements creates a higher strain on the cervical spine than the anterior twist alone and is a risk factor for neck lesions.8 ‑ 10 Also, a posture that includes bending of the upper body, lateral twist, and rotation, associated with prolonged and fixed tasks is a predisposing factor for lower back symptoms.11 Several studies in dentistry have investigated physical workload on the neck, houlders, and arms,7‑ 9,12 as well as wrists/hands8, 13‑ 15 during clinical activity.
Through ergonomics, dentists can modify and optimize their workspace, thus improving the work tasks. Ergonomic saddle seats are available in the market, and manufacturers claim they induce the adoption of a healthier posture. With a saddle seat, the pelvis rotates anteriorly, and the lumbar spine adopts the correct curvature, which decreases the risk of musculoskeletal problems while the dentist works.16 Some authors suggested that adjustable chairs that reduce flexion of the hips and promote a better lumbar spine posture are associated with less muscular tension.17 It is important to take ergonomics into consideration to maintain the ability and efficacy of the health care professional, which will improve patient care.18
The aim of this study is to compare dentists’ whole‑body posture when using a conventional seat chair versus a saddle‑seat chair while performing a previously defined dental work, based on information obtained using wireless inertial motion sensors. The null hypothesis to be tested was as follows: there are no differences between a conventional seat chair and a saddle‑seat chair in terms of dentists’ posture during dental work.
Materials and methods
The study was outlined according to the established legal norms (Helsinki Declaration; Additional Protocol to the Convention on Human Rights and Biomedicine – Strasbourg 2005; Law No. 12/2005) and was approved by the Faculty of Engineering of the University of Porto (Portugal). Twenty‑four volunteer dentists were included after informed, written consent. The dentists who worked on a conventional chair (KaVo, Germany) (Figure 1) were included in Group I (n=19), and the dentists who worked on a saddle‑seat chair (Salli, Finland) (Figure 2) were included in Group II (n=5).
The subjects’ ages ranged between 25 and 59 years old. The study was performed at a dental clinic equipped with dental phantom heads (KaVo, Germany), in Porto.
Every participant performed four dental tasks on a reclining dental phantom head (KaVo, Germany), as depicted in Figure 3.
The task selected for this study is
the most common dental procedure and is representative of general dentistry
practice. It consisted of a preparation of a tooth
cavity: Class I cavity in the upper right (1st quadrant) and left (2nd quadrant)
first molars and lower right (4th quadrant) and left (3rd quadrant) first molars.
This procedure involves removing all defective occlusal
pits and fissures from a tooth’s occlusal surface. The dentists’ posture and movements
were assessed using Xsens® MVN BIOMECH (Xsens Technologies BV, Enschede, Netherlands),
which is a full‑body inertial kinematic measurement system that
comprises 17 sensors and integrates 3D linear accelerometers, 3D gyroscopes, and 3D
magnetometers. These inertial units were attached
to the subject’s body using mounting straps. The units were placed, according
to the manufacturer’s specifications, on the head (using a headband), on the
8th thoracic vertebra, on the pelvis, and on both shoulders, upper arms,
forearms, hands (using gloves), upper legs, lower legs, and feet. A calibration procedure was
performed on each subject, in a magnetically‑sound
environment, before data acquisition. The reference position was N‑Pose, defined by standing upright on
a horizontal surface with face forward, parallel feet with one‑foot width apart, knees above feet,
hips above knees, straight back, shoulders above hips, straight arms alongside the
body (vertically), and thumbs forward. The movement parameters were sampled at
120 HZ. Every participant performed a Class
I cavity preparation on the first molar of each dental quadrant (Group I and
II), and the four tasks were observed. For further analysis, the most representative
posture during dental work was selected, and the joint angles of the head, shoulders,
elbows, wrists, trunk, pelvis, hips, and knees were registered for each dental
task within both groups. Data was analysed
using Visual 3D TM (C‑Motion,Inc., Rockville, MD, USA), Microsoft Excel
for Mac 2011 (Albuquerque, NM, USA), and IBM SPSS Statistics version 21
(Chicago, Illinois, USA). Due to the small sample size, the statistical
analysis was based on non‑parametric tests. For all measures, comparisons
were performed between the conventional seat and the saddle seat, for the four
tasks, using the Wilcoxon rank‑sum test. All comparisons were two‑tailed, and the significance level
was set at 5% (p < 0.05). Results Dentists tended to adopt a
pronounced forward‑tilted head position. In both groups, in all four
tasks, a high degree of forward head bending was detected (conventional chair,
47.9º; ergonomic chair, 47.2º). Regarding head rotation, dentists in a saddle
seat tended to rotate the head to a higher degree than dentists in a
conventional seat, but with no statistically significant differences. Lateral flexion of the head while
working on the upper right side of the jaw was similar between groups, with every
subject bending more than 25º to the right during this task. Work on the lower right side of the
jaw also showed the same results between groups, with the head bending
approximately 10º to the left side (Table 1). 


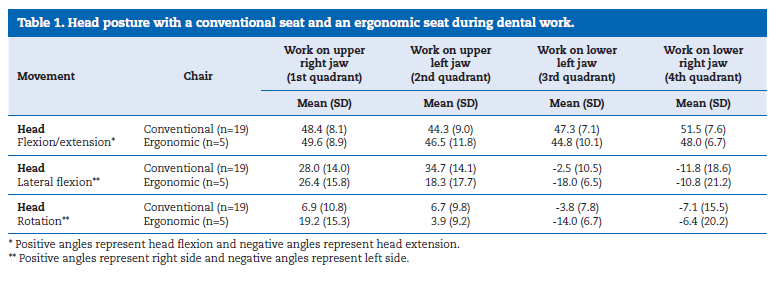
A 16º difference between groups was identified during work on the upper left side of the jaw. In this task, lateral flexion to the right side was more evident while working on a conventional seat than on a saddle seat. On the other hand, dentists on a saddle seat were more prone to bend the head to the left side while working on the lower left side of the jaw, when compared to dentists on a conventional seat. However, no statistical differences were found between groups.
Considering the trunk, subjects on an ergonomic chair showed less trunk flexion while working on the lower jaw.
Lateral flexion of the trunk was most evident with a conventional seat chair. Work on the lower left jaw showed high‑degree lateral flexion and trunk rotation to the right side in dentists on a conventional seat. There were no statistically significant differences between the groups regarding trunk position.
In the present study, significant statistical differences were identified between conventional and ergonomic seats concerning the upper arms working position. The right shoulder was more abducted in Group I than in Group II (p<0.05). This difference was quite evident while working on the lower jaw.
Right upper‑arm flexion was similar between groups (Table 2).
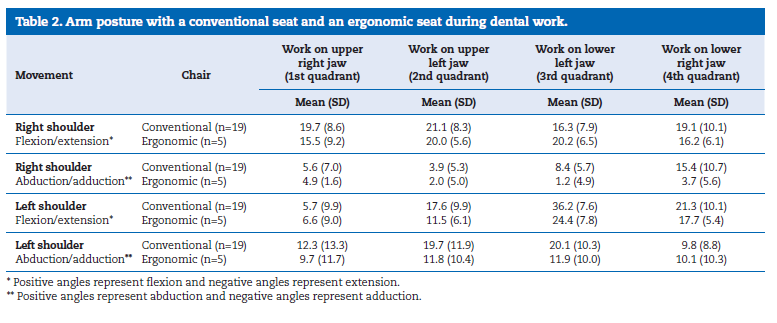
In all four tasks, right elbow joint angles were similar between groups.
The left shoulder was more abducted in Group I, especially while working on the left side of the mouth, with an 8º difference between groups. Left upper‑arm flexion was most evident in Group I. The main differences were observed when the dentists performed on the left side of the mouth. Significant differences were found in left elbow flexion, which was more pronounced with an ergonomic seat (p<0.05) during treatment in all dental quadrants.
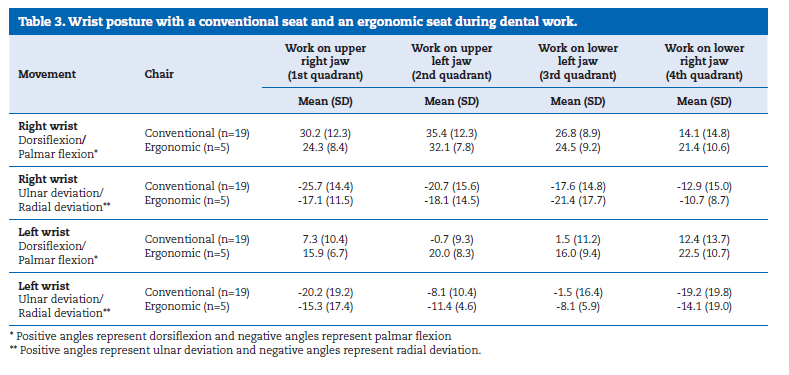
In this study, dentists showed more evident radial deviation and dorsiflexion in the right wrist than in the left wrist, during work. Differences were found between both seats (Table 3). Group I showed higher values of radial deviation and dorsiflexion of the right wrist than Group II, while working on the upper jaw. Dorsiflexion of the left wrist was statistically higher in the ergonomic seat group, with a difference of 20º when working on the 2nd quadrant (p<0.05) and a difference of 14º when working on the 3rd quadrant (p<0.05). In a general way, radial deviation of the left wrist was more evident in Group II.
Regarding the pelvis, two movements were studied: forward/backward rotation, which was described as anteversion/retroversion, and left and right elevation. Both groups lifted the pelvis to the left side while working on the upper jaw and to the right side while working on the lower jaw (Table 4). Regarding anteversion/retroversion, the dentists seated on an ergonomic seat showed more anteversion than the dentists on a conventional seat, while working on the lower jaw. Work on the upper jaw was similar between groups. No statistical differences were found between groups.
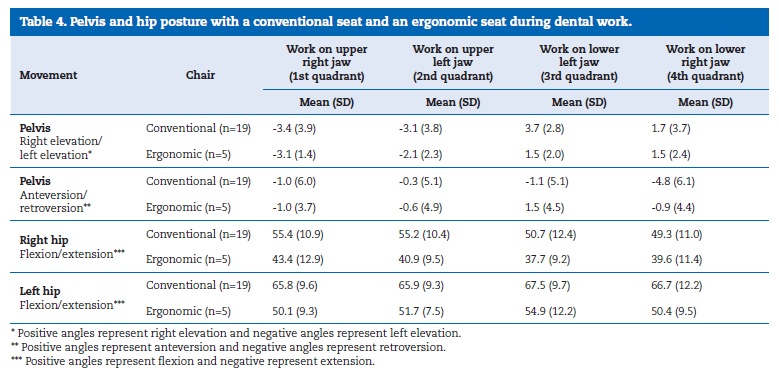
Dentists working on a saddle seat showed less hip flexion.
There were statistically significant differences between groups in both hip joint positions (p<0.05). Both groups flexed more the left hip than the right hip (Table 4), which could be explained by the use of the pedal, mostly performed with the left foot. No major differences were found in knee joint flexion in both groups.
Discussion
The results obtained in this study confirm that dental work is associated with excessive neck flexion and cervical rotation.
This finding is in accordance with other authors, who reported head bending between 17º and 39º in a group of dentists.8
Previous studies found that dentists worked with a forward head position, but not so pronounced as these results showed.5,10 Silva et al., in a preliminary study with the same method and Xsens technology, reported a neck flexion of 19º for all dental tasks.19 Although other studies 8 ,10,19 showed lower values of lateral head flexion, this study revealed an excessive head bent position in all four dental tasks while using the conventional and ergonomic seats. However no major differences were found in head flexion between the two chairs evaluated. Considering head rotation, dentists who worked on a saddle seat were more likely to rotate their head compared to dentists on a conventional seat. Even though no significant statistical differences were found, the ergonomic saddle seat seems to provide a better trunk position, with less forward and lateral flexion of the neck when compared to the conventional seat.
Previous studies in dentists10 and dental hygienists20 reported a high upper‑arm elevation, which is consistent with this study’s results. In the present study, dentists who worked on ergonomic chairs showed less arm flexion and abduction in both the left and right arm. Arm elevation should be reduced during dental work to prevent muscular injuries and upper‑arm symptoms.
Some authors found that the right hand was in a more dorsiflexed and deviated position than the left hand, in a group of female dentists.8 Other authors found similar results in a group of dental hygienists.20 In the present study, major statistical differences were identified between the right and the left hands, during all four dental procedures.
In both groups, the right hand was held in a more dorsiflexed position and more deviated to the radial side than the left one. This finding is consistent with the work of right‑handed dentists, as they use the left hand to ensure the visibility of the operating field and the right hand to execute the treatment.
This study revealed that dentists who used a conventional seat when working on both the upper and lower jaw of the dental phantom head had better left‑wrist posture than dentists who used an ergonomic seat. Some authors studied the effects of wrist posture on carpal tunnel pressure, and reported that this increases with postural deviations from the neutral position of the wrist. It is recommended that dentists avoid extreme wrist postures associated with static work.21
Others studied lumbar posture in three different dental chairs during a dental task, and showed that the pelvis was in a more flexed position on a conventional seat compared with a saddle seat.22 This study revealed similar results when dentists were working on the lower jaw. The use of a saddle seat results in a more lordotic posture due to the anteversion of the pelvis.
Regarding hip flexion, it was more pronounced with a conventional seat than with an ergonomic seat. These findings are in accordance with a saddle‑seat posture. Pynt defines an optimal sitting posture as a tilted anterior pelvis and hips with at least 60º of flexion, resulting in lordosis of the lumbar spine, which is recommended to maintain a healthy posture and to prevent lower back pain.23
In a general way, considering that the data were derived from the most representative dental work position, the results are consistent with other studies in dentistry. 5 , 8 , 10 , 20 However, the reduced number of volunteers working on a saddle‑seat chair was a major limitation of this study. Despite the revealing differences found between groups, the small sample size is a concern and, therefore, the results should be carefully interpreted while further studies are conducted.
Conclusions
A saddle seat seems to promote a healthy posture, regarding maintenance of lumbar lordosis, which is associated with lower disc pressure. Also, this study suggests that a saddle seat provides less physical workload to the arms and trunk during dental work.
Dentists need instruction and training on ergonomic principles, as well as more functional dental equipment. As a preventive measure, students should also be instructed to work with an ergonomic position and acquire good postural habits from the beginning of their career. Therefore, it is crucial to obtain objective data from a kinematic study of the dentists’ clinical activity using various dental ergonomic equipment.
Further studies are required to understand the role of ergonomics in dentistry and to confirm if the saddle‑seat chair or another ergonomic equipment improves the dentists’ body posture during dental work.
References
1. Newell TM, Kumar S. Prevalence of musculoskeletal disorders among orthodontists in Alberta. Int J Ind Ergon. 2004;33:99‑107.
2. Yamalik N. Musculoskeletal disorders (MSDs) and dental practice; Part 1. General information‚ aetiology, work‑relatedness, magnitude of the problem, and prevention. Int J Ind Ergon. 2006;56:359‑66.
3. Åkesson I, Johnsson B, Rylander L, Moritz U, Skerfving S. Musculoskeletal disorders among female dental personnel‑clinical examination and a 5‑year follow‑up study of symptoms. Int Arch Occup Environ Health. 1999;72:395‑403.
4. Åkesson I, Schütz A, Horstmann V, Skerfving S, Moritz U. Musculoskeletal symptoms among dental personnel;‑lack of association with mercury and selenium status, overweight and smoking. Swed Dent J. 2000;24:23‑38.
5. Finsen L, Christensen H, Bakke M. Musculoskeletal disorders among dentists and variation in dental work. Appl Ergon. 1998;29:119‑25.
6. Fish D, Morris‑Allen D. Musculoskeletal disorders in dentists. N Y State Dent J. 1998;64:44‑8.
7. Milerad E, Ekenvall L. Symptoms of the neck and upper extremities in dentists. Scand J Work Environ Health. 1990:129‑34.
8. Åkesson I, Hansson G‑ Å, Balogh I, Moritz U, Skerfving S. Quantifying work load in neck, shoulders and wrists in female dentists. Int Arch Occup Environ Health. 1997;69:461‑74.
9. Finsen L. Biomechanical aspects of occupational neck postures during dental work. Int J Ind Ergon. 1999;23:397‑406.
10. Jonker D, Rolander B, Balogh I. Relation between perceived and measured workload obtained by long‑term inclinometry among dentists. Appl Ergon. 2009;40:309‑15.
11. Andersson GB. Epidemiological features of chronic low‑back pain. Lancet. 1999;354:581‑5.
12. Green EJ BM. An aid to the elimination of tension and fatigue: body mechanics applied to the practice in dentistry. J Am Dent Assoc. 1963;67:679‑97.
13. Dong H, Barr A, Loomer P, Rempel D. The effects of finger rest positions on hand muscle load and pinch force in simulated dental hygiene work. J Dent Educ. 2005;69:453‑60.
14. Dong H, Barr A, Loomer P, LaRoche C, Young E, Rempel D. The effects of periodontal instrument handle design on hand muscle load and pinch force. J Am Dent Assoc. 2006;137:1123‑30.
15. Dong H, Loomer P, Barr A, LaRoche C, Young E, Rempel D. The effect of tool handle shape on hand muscle load and pinch force in a simulated dental scaling task. Appl Ergon. 2007;38:525‑31.
16. Gandavadi A, Ramsay J. Effect of two seating positions on upper limb function in normal subjects. Int J Ther Rehabil. 2005;12:485‑90.
17. Koskelo R, Vuorikari K, Hänninen O. Sitting and standing postures are corrected by adjustable furniture with lowered muscle tension in high‑school students. Ergonomics. 2007;50:1643‑56.
181. Gupta A, Manohar Bhat TM, Bansal N, Gupta G. Ergonomics in dentistry. Int J Clin Pediatr Dent. 2014;7:30‑4.
19. Silva V, Reis‑Campos J, Figueiral M, Fonseca P, Pinho M, Vaz M. Preliminary inertial study of body postures during dental procedures. Biodental Engineering III. 2014:287‑90.
20. Åkesson I, Balogh I, Hansson GÅ. Physical workload in neck, shoulders and wrists/hands in dental hygienists during a work‑day. Appl Ergon. 2012;43:803‑11.
21. Rempel DM, Keir PJ, Bach JM. Effect of wrist posture on carpal tunnel pressure while typing. J Orthop Res. 2008;26:1269.
22. De Bruyne MAA, Van Renterghem B, Baird A, Palmans T, Danneels L, Dolphens M. Influence of different stool types on muscle activity and lumbar posture among dentists during a simulated dental screening task. Appl Ergon. 2016;56:220‑6.
23. Pynt J, Higgs J, Mackey M. Seeking the optimal posture of the seated lumbar spine. Physiother Theory Pract. 2001;17:5‑21.
Vanessa Silva
E-mail address: vanessa.m.b.ss@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgements
The authors thank Manuel Neves, DDS, for providing his dental clinic equipped with dental phantom heads. The authors thank Ponto Médico Lda., for providing an ergonomic saddle-seat chair.
Article history:
Received 11 August 2016
Accepted 8 December 2016
Available online 30 March 2017