
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD | 2017 | 58 (4) | 219-224
Original research
Shear Bond Strength of different accessories used to traction impacted teeth
Resistência adesiva ao cisalhamento de diferentes acessórios utilizados para tração de dentes impactados
a Health I Department, Universidade Estadual do Sudoeste da Bahia – UESB, Jequié, Bahia, Brazil and Pediatric Dentistry and Orthodontic Department Universidade Federal do Rio de Janeiro-UFRJ, Rio de Janeiro, Rio de Janeiro, Brazil
b Health I Department, Universidade Estadual do Sudoeste da Bahia – UESB, Jequié, Bahia, Brazil
Matheus Melo Pithon - matheuspithon@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 58
Issue - 4
Original research
Pages - 219-224
Go to Volume
Article History
Received on 28/11/2016
Accepted on 29/09/2017
Available Online on 20/12/2017
Keywords
Original research
Shear Bond Strength of different accessories used to traction impacted teeth
Resistência adesiva ao cisalhamento de diferentes acessórios utilizados para tração de dentes impactados
Matheus Melo Pithona,*, Matheus Souza Campos Costab, Heitor Cesár Ribeiro de Almeida Júniorb, Ivanderson Santana de Almeidab, Benito Coelho Santanab, Raildo da Silva Coqueirob
a Health I Department, Universidade Estadual do Sudoeste da Bahia – UESB, Jequié, Bahia, Brazil and Pediatric Dentistry and Orthodontic Department Universidade Federal do Rio de Janeiro-UFRJ, Rio de Janeiro, Rio de Janeiro, Brazil.
b Health I Department, Universidade Estadual do Sudoeste da Bahia – UESB, Jequié, Bahia, Brazil.
http://doi.org/10.24873/j.rpemd.2017.12.032
ABSTRACT
Objectives: To evaluate the shear bond strength and the adhesive remnant index (ARI) of different orthodontic accessories used for applying traction on impacted teeth.
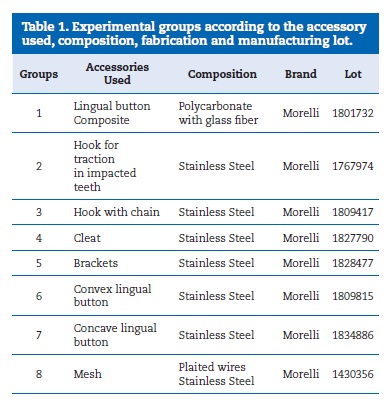
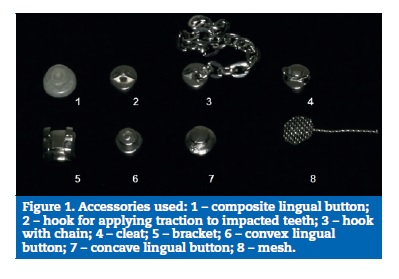
Methods: 120 bovine incisors were used. Initially, all teeth were submitted to prophylaxis, subsequent etching with 37% phosphoric acid, application of adhesive and light polymerization. Afterwards, these teeth were randomly divided into eight groups: (1) composite lingual button; (2) hook for application of traction on impacted teeth; (3) hook with chain; (4) cleat; (5) brackets; (6) convex lingual button; (7) concave lingual button; and (8) orthodontic mesh. The groups were submitted to shear tests in a universal test machine, and ARI evaluation.
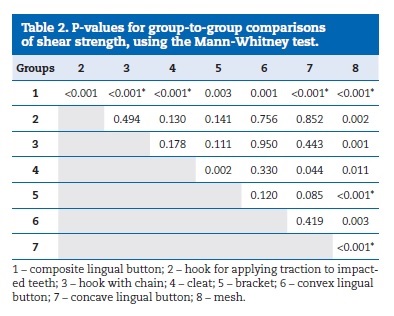
Results: The group of orthodontic mesh (8) presented the best shear bond strength results with statistically significant differences comparing with the composite lingual button (p<0.001), hooks for application of traction on impacted teeth (p=0.002), hooks with chain (p=0.001), cleat (p=0.011), brackets (p< 0.001), convex lingual button (p=0.003) and convex lingual button (p<0.001). The highest mean ARI values were also obtained for the mesh group, with statistically significant differences comparing with the composite lingual button (p=0.008), cleat (p=0.004), brackets (p=0.001), convex lingual button (p=0.017) and concave lingual button (p=0.005).
Conclusion: The greatest adhesion forces were obtained with the orthodontic mesh, which was statistically different from all other groups, and the lowest adhesion forces with the composite lingual button.
Keywords: Bond strength,Impacted, Orthodontic appliance, Tooth
RESUMO
Objetivos: Avaliar a resistência adesiva ao cisalhamento e o Índice de Adesivo Remanescente (IAR) de diferentes acessórios ortodônticos utilizados na tração de dentes impactados.
Métodos: 120 incisivos bovinos foram utilizados para esse estudo. Inicialmente, em todos realizou-se profilaxia, seguida do condicionamento com ácido fosfórico 37%, aplicação de adesivo e fotopolimerização. Em seguida, dividiu-se aleatoriamente os dentes em oito grupos: (1) Botão língual em resina composta; (2) Gancho para tracionar dentes inclusos; (3) Gancho com corrente; (4) Cleat; (5) Brackets; (6) Botão lingual convexo; (7) Botão lingual côncavo e (8) Malha metálica ortodôntica. Os grupos foram submetidos a testes de resistência adesiva ao cisalhamento em máquina de ensaios universais e avaliação do IAR.
Resultados: O grupo constituído pelas malhas metálicas ortodônticas apresentou os melhores resultados nos testes resistência adesiva ao cisalhamento com diferenças estatisticamente significativas quando comparados com os botões linguais em resina composta (p<0,001), Ganchos para tracionar dentes inclusos (p=0,002), Ganchos com corrente (p=0,001), Cleat (p=0,011), Brackets (p< 0,001), Botão lingual convexo (p=0,003) e Botão lingual côncavo (p<0,001). As maiores médias do IAR foram obtidos também pelo grupo das Malhas metálicas ortodônticas, com diferenças estatisticamente significativas quando comparadas aos Botões linguais em compósito (p=0,008), Cleat (p=0,004), Brackets (p=0,001), Botão lingual convexo (p=0,017) e Botão lingual côncavo (p=0,005).
Conclusões: As forças de adesão maiores foram obtidas com a malha ortodôntica, tendo sido estatisticamente diferente de todos os outros grupos e as menores com os botões linguais em compósito.
Palavras-chave: Adesão, Impactado, Aparelho ortodôntico, Dente
Introduction
Impacted teeth are a prevalent problem in the orthodontic treatment,1 and are defined as teeth that remain in the oral mucosa or bone after their period of eruption. 2 - 5 There are various causes for this anomaly, which may be due to an obstruction of the trajectory between its site of development and the functional occlusal position, or due to a loss of eruptive force.6
The methods described in the literature for the treatment of impacted teeth vary between extraction, autotransplantation and surgical exposure, with a subsequent orthodontic movement.9 The latter is the most recommended option, as it presents the best results from both the aesthetic and functional points of view.10 When the treatment option is the application of traction, it is necessary to adapt some accessory to the tooth in question, which will serve as a support for traction with orthodontic forces.11 In the past, this support was obtained using invasive methods, such as placing a wire loop around the crown10 or transfixation11 (the perforation of the incisal angle in the vestibular-lingual direction and fixation of an orthodontic wire). However, many complications resulted from these procedures, such as root resorptions and pulp perforations, with the need for future endodontic treatment. 8 , 12 , 13
Based on this premise, the authors’ proposal in the present study was to evaluate the in vitro shear bond strength and adhesive remnant index (ARI) of different orthodontic accessories used for applying traction to impacted teeth. In addition, the null hypothesis tested was that the shear bond strength and the ARI were similar for all orthodontic traction objects.
Materials and methods
In this in vitro evaluation, 120 bovine permanent incisors were used due to the similarity between bovine and human teeth. The inclusion criterion was that the teeth should be intact – that is, without cavitation caused by caries and/or the extraction process. The teeth were cleaned with water and stored in a glass receptacle in a 10% formaldehyde solution for seven days and kept refrigerated.
The minimum sample size required for this study was calculated using the following parameters: a test power of 80% (β=0.20) and an error of 5% (α>=0.05). The calculation determined a minimum sample size of 12 samples. Considering the possibility of using non-parametric statistics (Friedman test), an increase of 20% was applied, which resulted in the adjustment of the minimum size required for 15 individuals. The sample calculation was performed in G*Power (version 3.1.9.2, Germany).
The teeth were embedded in PVC rings (Tigre, Joinville, Brazil) with acrylic resin (Clássico, São Paulo, Brazil) so that only their crowns were exposed. In order to maintain the surface to be glued to the bracket perpendicular to the ground, a square was used for standardization. After polymerizing the resin, all the test specimens were stored in distilled water and again placed in the refrigerator at 5ºC.
The vestibular surfaces of the teeth received prophylaxis with a rubber cup (Viking, KG Sorensen, Barueri, Brazil), an extra-fine pumice stone (S.S.White, Juiz de Fora, Brazil) and distilled water for 15 seconds. Afterwards, they were washed with air spray/distilled water and dried with oil- and humidity-free jets of air for the same length of time. After prophylaxis, etching was performed with 37% phosphoric acid (FGM, Joinville, Brazil) for 30 seconds, followed by washing with water and drying with jets of air for the same period. A thin coat of primer (Transbond XT; 3M Unitek, Monrovia, California, USA) was applied and light polymerized for 40 seconds.
Before the bonding process, the teeth were randomly divided into groups corresponding to the accessory that would be bonded to them, as shown in Table 1 and Figure 1.
An orthodontic composite (Transbond XT, Monrovia, USA) was used for bonding. Initially, composite was applied on the base of the accessories, which were then placed on the tooth surface and subjected to a force of 300g, to allow extravasation of the excess composite. For this purpose, a weight of 300 g was positioned on top of the brackets. The excess composite was removed with an exploratory probe no. 5.
The mesh was previously standardized so that it would always have the same dimensions, and the same amount of orthodontic composite would be applied. For this purpose, the internal diameter of an orthodontic elastic (3.1 mm) was used to delimit the cross-sectional area of the mesh. Afterwards, the mesh was placed on the tooth surface coupled with an elastic, and the interior of the elastic was filled with orthodontic composite (Transbond XT, Monrovia, USA).
The next step was light polymerization for 40 seconds with the light-polymerization device XL 1500 (3M Unitek, Monrovia, CA, USA), using a light intensity of 400 mW/cm², regularly checked with a radiometer (Demetron, Danbury, CT, USA).
After bonding, the test specimens were stored in artificial saliva and kept in an oven at a temperature of 37°C for 24 hours. The bond strength tests were performed in a universal mechanical test machine (AME-2kN; Fillizola, São Paulo, Brazil), operating at a speed of 0.5 mm/min, by means of a chisel-shaped active tip. The shear strength forces were obtained in kilogram-force, converted into Newton, and divided by the base area of the tested accessory. Thus, the results were given in megapascal (MPa). Megapascal was the chosen unit because it allowed individualizing the force applied on a specific area in mm², thereby annulling the variable corresponding to the base area of each accessory tested.
After performing the shear strength tests, the vestibular surfaces of the tested specimens were evaluated under a stereomicroscope (Carl Zeiss, Göttingen, Germany), at 16x magnification, to quantify the ARI. The ARI scores ranged from 0 to 3, with 0 indicating that there were no composite remnants on the enamel, 1 that there was less than half of the composite, 2 that there was more than half of the composite and 3 that the whole composite was on the tooth surface.
The means and standard deviations were calculated for the descriptive analysis of the shear strength and ARI. For the inferential analysis of the shear strength, the homogeneity of variances was tested using the Levene’s test and the normality of the residues using the analysis of variance (one-way ANOVA), namely, the Kolmogorov-Smirnov test. After verifying the heterogeneity of variances and the asymmetrical distribution of the residues, the Kruskal-Wallis test was applied to compare differences between the groups; the comparisons between pairs were made using the Mann-Whitney test. The Kruskal-Wallis and Mann-Whitney tests were also used to verify the differences in ARI scores between the groups. The adopted level of significance was 5% (α=0.05). The data were tabulated and analyzed in the software program IBM SPSS Statistics for Windows (IBM SPSS. 21.0, 2012, Armonk, NY: IBM Corp.).
Results
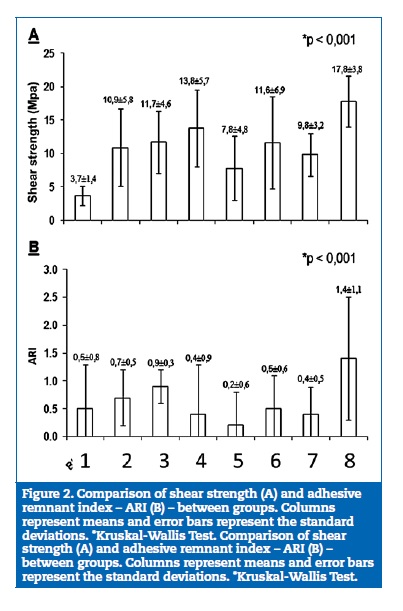
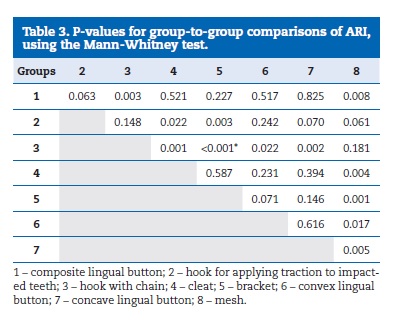
Based on the results, it was demonstrated that the mesh (Group 8) was the accessory that resulted simultaneously in the highest shear strength values and highest ARI scores. (Figure 2). The shear strength of the mesh differed statistically from that of all other materials (Table 2) and its ARI score did not differ only from the hook for applying traction to impacted teeth and the hook with chain (Table 3). The lowest shear strength was observed with the use of the composite lingual button (Group 1) (Figure 2A), which differed statistically from all other materials (Table 2). The lowest ARI values were observed with the use of brackets (Figure 2B), which differed statistically from the hook for applying traction to impacted teeth, the hook with chain and the mesh (Table 3).
Discussion
Various devices have been designed for bonding to the enamel of a tooth to which orthodontic traction will be applied. 14 , 17 Choosing a device depends on individual preferences since there is no scientific proof in the literature, up to the present moment, indicating which accessory best adheres to the tooth surface, in order to avoid debonding during the application of traction and the need for a new surgical intervention. 7 , 8
Therefore, the forces used for applying traction to impacted teeth range between the values of 20-150 grams-force. 21 - 23
In
all the groups tested, this value was achieved when the means were evaluated,
except in the composite lingual button group (mean = 3.7 MPa).
This fact may be explained by the composition of this accessory, consisting of
polycarbonate with glass fiber. Some studies have analyzed orthodontic
accessories constituted by this composite and have proved that, when compared
with other metal orthodontic accessories, these have a lower bond strength than
the metal type.
24
-
26
Furthermore,
it is pointed out that this value shows a trend to decrease in clinical
situations since some elements such as saliva and blood are present, and thus
make it difficult to bond orthodontic accessories to tooth enamel.
27
It should be emphasized that the only group in which all specimens showed results above the reference value was the group with the orthodontic mesh, which presented statistically significant differences comparing with all the other groups.
Although a bond strength of over 14 MPa may cause damage to the tooth surface,33 this did not occur in any specimen of the mesh group, as opposed to the group of the hook for applying traction to impacted teeth (GTDI), in which two specimens presented enamel fractures. This fact may be explained by the design of the base of these orthodontic accessories.
Regarding the ARI, the best results were also obtained in the orthodontic mesh group (mean = 1.4), thus ratifying that orthodontic accessory bonding is most effective when a failure occurs by cohesive rupture of the material; that is, when adhesive remnants are found adhered to the tooth.34 The worst results were found in the bracket group (mean = 0.2), and this group presented statistically significant differences in comparison with the hook for applying traction to impacted teeth (GTDI), the hook with chain (GC) and the mesh.
The favorable results found for the orthodontic mesh bring to light the strong correlation between the bond strength at the adhesive-enamel interface and the ARI.35 Furthermore, other advantages may be pointed out, such as the possibility of using it when the teeth are in critical positions, its simplicity, its low cost, being easy to fit to tooth surfaces (vestibular, palatine, lingual, mesial or distal) and providing less discomfort.36
The limitation of this study is that it was conducted in vitro, therefore excluding some important variables arising in the clinical practice that have a direct influence on the bond of accessories to the surface of a tooth that will be submitted to traction. Therefore, clinical studies are necessary to determine whether the results obtained in the laboratory are consistent with the reality experienced in the clinical practice.
Conclusion
By conducting this study, it could be concluded that:
– the polycarbonate and glass fiber button did not show good strength when applying traction to impacted teeth;
– stainless steel accessories showed good strength and are indicated for applying traction to impacted teeth;
– orthodontic mesh presented the best results both in shear strength tests and in the adhesive remnant index;
– brackets showed the worst results in the adhesive remnant index;
– the hypothesis was rejected since the accessories presented different strengths of resistance.
REFERENCES
1. Correia LP, Pinho MM, Manso MC. Motivation, perception of the impact and level of satisfaction with orthodontic treatment. Rev Port Estomatol Med Dent Cir Maxilofac. 2016;57:247-51.
2. Kim Y, Hyun HK, Jang KT. The position of maxillary canine impactions and the influenced factors to adjacent root resorption in the Korean population. Eur J Orthod. 2012;34:302-6.
3. Jung YH, Kim JY, Cho BH. The effects of impacted premaxillary supernumerary teeth on permanent incisors. Imaging Sci Dent. 2016;46:251-8.
4. Ghaeminia H, Perry J, Nienhuijs ME, et al. Surgical removal versus retention for the management of asymptomatic disease-free impacted wisdom teeth. Cochrane Database Syst Rev. 2016:CD003879.
5. Saponaro G, Pelo S, De Angelis P, Forcione M, D’Amato G, Moro A. Bone Flap Technique for Impacted Teeth Extraction and Bone Cysts Removal. J Craniofac Surg. 2016;27:1084-6.
6. Rajendran R. Shafer’S Textbook Of Oral Pathology (6Th Edition): Elsevier (A Divisionof Reed Elsevier India Pvt. Limited); 2009.
7. Maló L, Cabrita A, Rafael A. Orthodontic movement; evaluation of periodontal ligament in a experimental study on adult Wistar rats. Rev Port Estomatol Med Dent Cir Maxilofac. 2014;55:152-8.
8. Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992;101:159-71.
9. de Oliveira MV, Pithon MM. Attempted traction of impacted and ankylosed maxillary canines. Am J Orthod Dentofacial Orthop. 2012;142:106-14.
10. McBride LJ. Traction–a surgical/orthodontic procedure. Am J Orthod. 1979;76:287-99.
11. Fournier A, Turcotte JY, Bernard C. Orthodontic considerations in the treatment of maxillary impacted canines. Am J Orthod. 1982;81:236-9.
12. Boyd RL. Clinical assessment of injuries in orthodontic movement of impacted teeth. II. Surgical recommendations. Am J Orthod. 1984;86:407-18.
13. Arici N, Bulut E. Shear bond strength of orthodontic attachments bonded to impacted teeth under in vivo and in vitro conditions. Orthod Craniofac Res. 2014;17:170-7.
14. Hammad SM, El-Wassefy N, Maher A, Fawakerji SM. Effect of nanotechnology in self-etch bonding systems on the shear bond strength of stainless steel orthodontic brackets. Dental Press J Orthod. 2017;22:47-56.
15. Artun J, Bergland S. Clinical trials with crystal growth conditioning as an alternative to acid-etch enamel pretreatment. Am J Orthod. 1984;85:333-40.
16. Abu-Alhaija E, Jaradat M, Alwahadni A. An Ex-vivo Shear and tensile bond strengths of orthodontic molar tubes bonded using different techniques. J Clin Exp Dent. 2017;9:e448-e53.
17. Arash V, Naghipour F, Ravadgar M, Karkhah A, Barati MS. Shear bond strength of ceramic and metallic orthodontic brackets bonded with self-etching primer and conventional bonding adhesives. Electron Physician. 2017;9:3584-91.
18. Cossellu G, Lanteri V, Butera A, Laffi N, Merlini A, Farronato G. Timing considerations on the shear bond strength of orthodontic brackets after topical fluoride varnish applications. J Orthod Sci. 2017;6:11-5.
19. Reynolds I, Von Fraunhofer J. Direct bonding in orthodontics: a comparison of attachments. J Orthod. 1977;4:65-9.
20. Pithon MM, Batista VO, D’El Rey NC. Effect of different methods for decontaminating tooth enamel after contact with blood before bonding orthodontic buttons. J Oral Maxillofac Surg. 2012;70:2035-40.
21. Becker A, Shpack N, Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. Eur J Orthod. 1996;18:457-63.
22. Crescini A, Nieri M, Buti J, Baccetti T, Mauro S, Prato GP. Short- and long-term periodontal evaluation of impacted canines treated with a closed surgical-orthodontic approach. J Clin Periodontol. 2007;34:232-42.
23. Wisth PJ, Norderval K, Boe OE. Periodontal status of orthodontically treated impacted maxillary canines. Angle Orthod. 1976;46:69-76.
24. Caprioglio A, Fontana M, Longoni E, Cozzani M. Long-term evaluation of the molar movements following Pendulum and fixed appliances. Angle Orthod. 2013;83:447-54.
25. Guan G, Takano-Yamamoto T, Miyamoto M, Hattori T, Ishikawa K, Suzuki K. Shear bond strengths of orthodontic plastic brackets. Am J Orthod Dentofacial Orthop. 2000;117:438-43.
26. Liu JK, Chang LT, Chuang SF, Shieh DB. Shear bond strengths of plastic brackets with a mechanical base. Angle Orthod. 2002;72:141-5.
27. Pithon MM, Oliveira MV, Ruellas AC, Bolognese AM, Romano FL. Shear bond strength of orthodontic brackets to enamel under different surface treatment conditions. J Appl Oral Sci. 2007;15:127-30.
28. Hobson RS, Ledvinka J, Meechan JG. The effect of moisture and blood contamination on bond strength of a new orthodontic bonding material. Am J Orthod Dentofacial Orthop. 2001;120:54-7.
29. Xie J, Powers JM, McGuckin RS. In vitro bond strength of two adhesives to enamel and dentin under normal and contaminated conditions. Dent Mater. 1993;9:295-9.
30. Sayinsu K, Isik F, Sezen S, Aydemir B. Light curing the primer-beneficial when working in problem areas? Angle Orthod. 2006;76:310-3.
31. Faltermeier A, Behr M, Rosentritt M, Reicheneder C, Mussig D. An in vitro comparative assessment of different enamel contaminants during bracket bonding. Eur J Orthod. 2007;29:559-63.
32. Sayinsu K, Isik F, Sezen S, Aydemir B. Effect of blood and saliva contamination on bond strength of brackets bonded with a protective liquid polish and a light-cured adhesive. Am J Orthod Dentofacial Orthop. 2007;131:391-4.
33. Protásio MF, Frota PHD, Costa JF, Carneiro KK, Bauer J. Effects of application mode of self-etching primer on shear bond strength of orthodontic brackets. Rev Port Estomatol Med Dent Cir Maxilofac. 2016;57:9-13.
34. Eminkahyagil N, Arman A, Cetinsahin A, Karabulut E. Effect of resin-removal methods on enamel and shear bond strength of rebonded brackets. Angle Orthod. 2006;76:314-21.
35. Matasa CG. Adhesion and its ten commandments. Am J Orthod Dentofacial Orthop. 1989;95:355-6.
36. Scougall Vilchis RJ, Yamamoto S, Kitai N, Hotta M, Yamamoto K. Shear bond strength of a new fluoride-releasing orthodontic adhesive. Dent Mater J. 2007;26:45-51.
37. Ferraro-Bezerra M, Pouchain EC, Tavares RN, Soares EC. A simple device for traction of impacted teeth: a technical note. J Oral Maxillofac Surg. 2012;70:2278-9.
Matheus Melo Pithon
Correio eletrónico: rmatheuspithon@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgments
The authors thank the help of Diego Adrini Carvalho de Souza and Monique Santos Albuquerque during the confection of the samples.
Article history:
Received 28 November 2016
Accepted 29 September 2017
Available online 20 December 2017