
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD - Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2023 | 64 (4) | 162-169
Original research
Communication between dentists and dental technicians in Lisbon for the construction of removable partial dentures’ metal frameworks
Comunicação entre médicos dentistas e técnicos de prótese em Lisboa para a realização de esqueletos metálicos de próteses parciais removíveis
a Universidade de Lisboa, Faculdade de Medicina Dentária, Unidade de Investigação e Ciências Orais e Biomédicas (UICOB), Lisbon, Portugal
b Faculdade de Medicina Dentária da Universidade de Lisboa, Lisbon, Portugal
c Laboratório de Instrumentação, Engenharia Biomédica e Física da Radiação (LIBPhys), Lisbon, Portugal
Isabel Gomes - isabel.gomes@fmd.ulisboa.pt
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 64
Issue - 4
Original research
Pages - 162-169
Go to Volume
Article History
Received on 12/08/2023
Accepted on 12/12/2023
Available Online on 30/01/2024
Keywords
Original Research
Communication between dentists and dental technicians in Lisbon for the construction of removable partial dentures’ metal frameworks
Comunicação entre médicos dentistas e técnicos de prótese em Lisboa para a realização de esqueletos metálicos de próteses parciais removíveis
Isabel Gomes1* 0000-0002-9509-7495
Filipa Reis2 0009-0008-5708-4440
Teresa Mendes1 0000-0001-6232-0251
Luís Miguel Pires Lopes1,3 0000-0001-8633-827X
1 Universidade de Lisboa, Faculdade de Medicina Dentária, Unidade de Investigação e Ciências Orais e Biomédicas (UICOB), Lisbon, Portugal
2 Faculdade de Medicina Dentária da Universidade de Lisboa, Lisbon, Portugal
3 Laboratório de Instrumentação, Engenharia Biomédica e Física da Radiação (LIBPhys), Lisbon, Portugal
Article history:
Received 8 August 2023
Accepted 12 December 2023
Available online 30 December 2023
Abstract
Objectives: To evaluate the communication between dentists and dental technicians in Lisbon for the construction of metal frameworks for removable partial dentures (RPDs).
Methods: This observational study’s target population was laboratories in Lisbon. Data were collected through a questionnaire including six categories: medical prescription, conventional definitive impression and its disinfection, digital impression, analysis of study and working casts, and design and construction of the metallic structure. Dental technicians completed the questionnaire after consulting the medical instructions and observing the stone casts. The variables were subjected to descriptive statistics.
Results: Three laboratories agreed to participate in this study, and the final sample included 53 entirely completed questionnaires. All definitive casts were obtained by conventional impression, with a universal tray (67.9%) and alginate (84.9%). The laboratories disinfected all impressions, mostly with sodium hypochlorite (98.1%), and the dental technician analyzed 84.9% of the casts in the parallelometer. There were no pre-prosthetic preparations in 66% of the working casts. The dentists provided design instructions in five cases, and only one delivered a drawing on paper. All metal frameworks were made in cobalt-chromium, mainly by electronic induction casting (96.6%).
Conclusions: The dentist did not provide the dental technician with most of the design and planning instructions required for constructing removable partial dentures. This finding confirms the lack of communication between clinics and laboratories in Lisbon.
Keywords: Cobalt-chromium alloys, Communication, Dental clinics, Dental laboratories, Dental prosthesis, Removable partial denture
Resumo
Objetivos: Avaliar a comunicação entre médicos dentistas e técnicos de prótese dentária em Lisboa para a confeção de uma estrutura de prótese parcial removível esquelética.
Métodos: Foi realizado um estudo observacional cuja população-alvo foram laboratórios na área metropolitana de Lisboa. A recolha de dados foi realizada através de um questionário, que recolheu informação de 6 categorias: guia de requisição médica, impressão definitiva convencional e respetiva desinfeção, impressão digital, análise dos modelos de estudo e de trabalho, e desenho e construção da estrutura metálica. O preenchimento do questionário foi realizado pelos técnicos de prótese com consulta das requisições médicas e dos modelos de gesso. Foi realizada estatística descritiva das variáveis.
Resultados: Três laboratórios aceitaram participar no estudo. A amostra incluiu 53 questionários completamente preenchidos. Todos os modelos definitivos foram obtidos por impressão convencional, com moldeira universal (67,9%) e alginato (84,9%). Todas as impressões foram desinfetadas no laboratório, maioritariamente com hipoclorito de sódio (98,1%). A análise com paralelómetro foi realizada pelo técnico de prótese em 84,9% dos casos e 66% dos modelos de trabalho não tinham preparações pré-protéticas. Verificou-se que o médico dentista transmitiu instruções sobre o desenho em 5 casos e apenas num caso enviou o desenho em papel. Todas as estruturas metálicas foram obtidas em cobalto-crómio e o método mais usado foi a fundição por indução eletrónica (96,6%).
Conclusões: A maior parte das instruções do desenho e do planeamento para a construção de próteses parciais removíveis não foram fornecidas pelo médico dentista ao técnico de prótese dentária, verificando-se uma comunicação insuficiente entre clínicas e laboratórios em Lisboa.
Palavras-chave: Ligas com cobalto-crómio,Comunicação, Clínica dentária,Laboratório de prótese dentária,Prótese dentária,Prótese parcial removível
Introduction
In recent years, the population of partially dentate adults has increased compared to fully edentulous ones.1 - 3 According to the 2022 oral health barometer, 48.5% of the Portuguese population has 1 to 8 teeth missing, and 6.4% are completely edentulous.2
Edentulous spaces can be rehabilitated with fixed bridges, implant-supported prostheses, or removable prostheses. A removable partial denture (RPD) with a metal framework is often the simplest and most cost-effective solution for treating patients with multiple edentulous areas.3 - 8
According to the European Union Medical Device Regulation, removable prostheses are considered medical devices.9 Thus, the ethical and legal guidelines indicate that, in the fabrication of an RPD, the dentist is responsible for planning and prescribing the prosthesis and giving the laboratory all the necessary instructions for its manufacture according to the prescribed design.4 - 6, 8, 10 Principles of good practice indicate that fabricating an RPD requires a team approach involving the clinician, the dental technician (DT), and the patient.10
The dentist must inform the DT about the following parameters for RPD construction: the abutment teeth’s periodontal status, the patient’s expectations, and aesthetic
parameters. The dentist should also include pre-prosthetic preparations in its planning, which are essential for a successful treatment. In turn, the DT may analyze other parameters in a parallelometer, such as the parallelism of abutment teeth and undercut areas, and transmit them to the dentist.4 - 7 10
However, the literature shows that the above is not happening in clinical practice. In Ireland, Lynch and Allen reported that 53% of RPD prescriptions received by DTs did not include a design of the metallic structure.3 In Saudi Arabia, Nassani and Alotaibi7 concluded that 64.2% of RPD cases were planned exclusively by the DT. In the United Kingdom, Rice et al.10 observed that 48% of RPD prescriptions did not include occlusal rests, and 30% of the prescriptions that did (51.5%) did not have rest seats in the casts. In Portugal, Caniço5 and Alves6 reported that the DT did not receive design instructions from the dentist in 80% of the cases in Porto and 90.9% of cases in Lisbon, respectively. Thus, although communication between the laboratory and the clinic is essential, it is often insufficient, ambiguous, or even neglected.
This study aimed to evaluate the communication between the dentist and the DT for RPD framework construction by collecting data about fabrication methods and design from Lisbon dental laboratories.
Material and methods
This observational study’s target population was dental laboratories in Lisbon. Written invitations were sent to laboratories that fabricate RPDs in November 2021. All laboratories that voluntarily agreed to participate were included in the study. The study was previously approved by the Ethics Committee of the Faculty of Dental Medicine of the University of Lisbon (October 2021).
Study data were collected through a questionnaire adapted from the one Avrampou et al.4 applied to a Greek population in 2011. The adaptation included adding questions about digital impression and CAD-CAM techniques and removing questions about prosthesis components for RPDs (because the original questionnaire is very long). Three experts (oral health professionals and researchers with experience in questionnaire construction) reviewed the adaptation by verifying the questions’ relevance and clarity. Afterward, a pre-test with one laboratory confirmed the questionnaire’s applicability (December 2021). All laboratories received instructions on how to complete the questionnaire and completed three questionnaires in the presence of the researcher.
The questionnaire included 19 multiple-choice questions about RPD’s design process and fabrication, namely related to the dentists’ prescriptions (2 questions), definitive impression (1 question), conventional impression and its disinfection (5 questions), digital impression (2 questions), cast analysis (2 questions), design (4 questions), and metallic framework (3 questions). A DT filled out a questionnaire for each RPD case with a metal framework after analyzing the dentist’s prescription and the cast. The questionnaire was available for the laboratories between February and April 2022.
Statistical analysis was performed with SPSS version 29.0 (IBM SPSS Statistics, New York, NY, USA). It included descriptive statistics, namely all variables’ absolute and relative frequencies.
Results
Only three of the previously invited laboratories agreed to participate voluntarily. They were established in three parishes of the municipality of Lisbon: Alvalade (lab A), Campolide (lab B), and Olivais (lab C).
After rejecting all questionnaires that were incomplete or had incoherent answers, the sample consisted of 53 entirely completed questionnaires: 16 from lab A, 14 from B, and 23 from C. Each questionnaire was completed based on a single case’s prescription, impression, and cast.
Most prescriptions (62.3%), all in a laboratory form, were sent by general dentists (Table 1). The identifying information in the prescriptions was mostly identification of the patient by name (81.1%), followed by dates of start and delivery of the prosthesis (34%), coded identification of the patient (28.3%), and name and address of the laboratory (18.9%). Only one of the guides had the dentist’s signature and professional card number. Two requests did not include identifying information (Figure 1, Table 2).
Table 1. Training level of the requesting dentist (n=53).

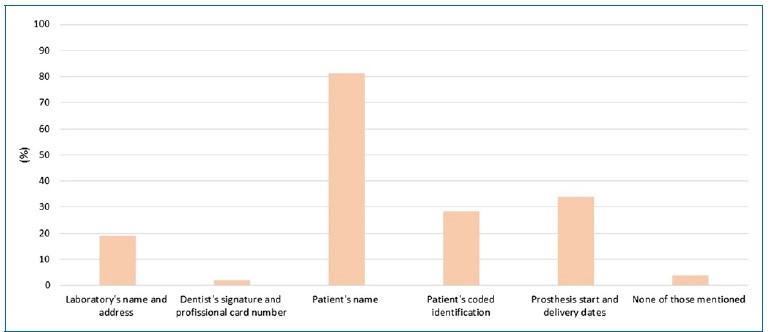
Figure 1. Frequency of information included in medical prescriptions.
Table 2. Frequency and type of identifying information in the prescriptions (n=53).

All casts for RPD manufacture were obtained by conventional impression (100%); no case used digital impression. Alginate was the most used impression material (84.9%), followed by elastomers (13.2%). Definitive impressions were made just with a universal tray in 67.9% of the cases (Figure 2, Table 3). All laboratories disinfected every impression received, regardless of having information on prior disinfection in the dental clinic. The prescriptions did not give that information in 20.8% of cases. The material most used by laboratories for disinfecting impressions was a solution of sodium hypochlorite (98.1%) (Figure 3, Table 4).

Figure 2. A) Impression material used for definitive impression; B) Tray used for fabricating removable partial dentures.
Table 3. Type of impression material and tray used (n=53).


Figure 3. Disinfection of the impressions: A) information on previous disinfection; B) disinfection in the laboratory; and C) type of disinfection material.
Table 4. Results related to the disinfection of impressions (n=53).

In 84.9% of the cases, the DT analyzed the casts in the parallelometer (Figure 4). Moreover, the DT planned the design for the RPD construction in 98.1% of the cases. The dentist and the DT did not work together in planning the design in any of the cases. In addition to the prescription, the dentist gave the laboratory instructions on the design of the skeletal RPD in five cases, mostly via telephone/mobile phone (7.5%). In one case, the dentist provided a drawing of the RPD structure on paper, with design instructions for the larger connector and the clasps of the metallic structure (Table 5).
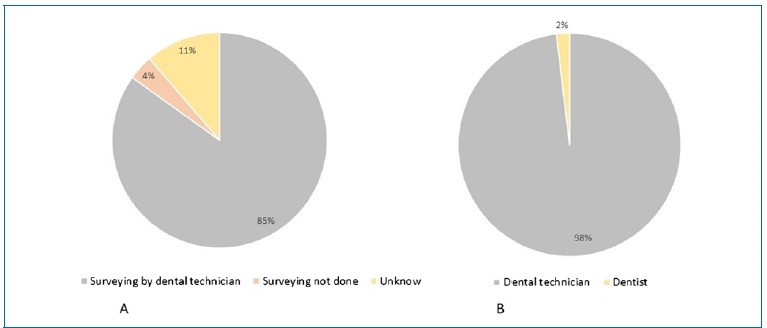
Figure 4. Professionals responsible for A) the surveying process and B) the design of prostheses.
Table 5. Results related to cast analysis in the parallelometer and design planning (n=53).

Only 34% of the working casts had pre-prosthetic preparations. These cases included preparations for occlusal and cingular rests (34%) and lingual and proximal guide planes (5.7%) (Figure 5, Table 6).
All RPD metallic structures manufactured in the laboratories were produced from cobalt-chromium alloys (Co-Cr), and most were manufactured by electronic induction casting (96.6%).

Figure 5. A) Frequency of pre-prosthetic preparations; B) Pre-prosthetic preparations identified on casts by type.
Table 6. Frequency of pre-prosthetic preparations (n=53).

Discussion
Not all laboratories can fabricate Co-Cr RPDs because the necessary equipment implies significant financial costs. Thus, they often forward these works to central laboratories, usually in large cities. Therefore, we analyzed laboratories in Lisbon. Teamwork and communication between the laboratory and the clinic are essential for constructing RPDs. The dentist is responsible for including instructions for the RPD fabrication in the prescriptions,11 as well as the laboratory’s name and address, the dentist’s signature and professional ID number, the patient’s identification by name or code, and the prosthesis’ start and delivery dates.9, 11, 12 In the present study, none of the prescriptions contained all that information, and two had no information. These alarming data indicate that prostheses are being manufactured without information identifying the patient and the prescriber. Thus, none of the involved professionals can be legally charged if problems arise during RPD’s transport, planning, or manufacture.4 - 6, 8, 10 Furthermore, the work might not be delivered, and the patient’s trust in the dentist may be compromised. The failure to send all legally necessary information in practice may result from dentists completing the prescriptions for the laboratory between appointments, with limited time. Given these worrying results, using a digital form that can only be sent once all mandatory fields are completed may be the best solution.
Definitive impressions must reproduce all the anatomical and morphological characteristics of the mucosa and abutment teeth.13, 14 They can be obtained by conventional techniques, impression materials, or digital technology.15 Intraoral scanning provides greater comfort for patients with vomiting reflex,15 reduces laboratory time, eliminates possible material distortions,15, 16 and allows storing digital data and repeating the prosthesis if necessary.14 Nevertheless, this study’s prescriptions only reported the conventional method. This prevalence may be related to intraoral scanners’ high costs17 and inability to allow functional impressions.15, 17 Similarly, Perti et al. reported digital printing use in only 1.39% of the cases.18
Alginate was the most used impression material in the definitive impressions (84.9%). This result agrees with one study in Portugal, in which all definitive impressions were made with alginate,5 and another in England, in which alginate was used in 59% of the impressions.18 Alginate is commonly used because it is easy to handle and less expensive than other available impression materials.13, 18 Despite offering poor detail reproduction, it reproduces the teeth and mucosa characteristics required for RPD framework construction.13 19
In this study, only 32.1% of the definitive impressions were obtained with individual trays, which is a low percentage compared to other studies: 82% in Caniço,5 and 60% in Kilfeather.19
Universal trays that are rigid enough and cover all the required structures are suitable for preliminary and definitive impressions.20 However, individual trays are preferable for dental preparations, which are required in RPDs.18
Regarding impression disinfection, the laboratories only had information on previous disinfection in 20.8% of cases and disinfected the impression in 100%, using sodium hypochlorite in 98.1%. The dentist must disinfect the impressions and inform the laboratory accordingly to protect the DT and reduce cross-contamination.5, 6, 17, 21 DTs unaware of previous disinfection may disinfect the impression again - double disinfection - thus reducing detail reproduction and the precision of the impression.21, 22, 23
Analyzing the study casts in the parallelometer is essential for RPD framework planning.19, 24, 25 This analysis should be followed by framework design and pre-prosthetic preparations in the oral cavity before the definitive impression.19 In this study, the DT analyzed the cast in the parallelometer in 84.9% of the cases. These results agree with the study by Caniço,5 where the DT did this in all cases. Ideally, the cast should be returned to the dentist after the DT’s parallelometer analysis for the subsequent planning and design of the structure.19
However, although the questionnaire did not specifically ask about it, we assume that did not happen because the RPD framework was designed by the DT in 98.1% of the cases. Pre-prosthetic preparations prevent horizontal loads o the abutment teeth, reduce food impaction, and improve the prostheses’ stability and retention.10, 24, 25 In this study, 66% of working casts had no prosthetic dental preparation, and only 34% had preparations for occlusal and cingular rests. These data agree with Rice et al.’s study,10 where only 30% of the casts had occlusal rest preparations.
In the present study, the DT planned the RPD design in 98.1% of the cases, which is a very high frequency compared to the literature, namely 54% in Kilfeather’s study.19 These data are alarming because they indicate a lack of instructions and clinical information regarding abutment teeth, which may lead to an inaccurate design of the RPD components, resulting in a dysfunctional RPD.5, 6, 7, 25
The results show that few dentists transmitted information about the RPD design planning, mostly via cell phone/ telephone (7.5%), and only one designed the framework and sent the drawing on paper. Similarly, in Caniço’s study,(5) the dentist planned the design in only one case, and in Alves’ study,6 90.9% of the prescriptions had no information about the major connector. Failure to send the design planning may result from a common incorrect practice of delegating the prescription filling to the assistant.
Co-Cr and titanium (Ti) alloys are the most used materials for RPD construction due to their high mechanical strength, high stiffness, and corrosion resistance.26 In the present study, all frameworks were produced using Co-Cr alloys. Similarly, Avrampou4 reported that 88.6% of frameworks were manufactured in Co-Cr alloys. In this investigation, 90.6% of the frameworks were produced by electronic induction casting, and the remaining 9.4% by hand casting. Processing Ti alloys by conventional casting techniques is difficult,27 and no frameworks were produced by CAD/CAM systems using laser sintering in this study. Metallic structures produced with the digital workflow have shown good adaptation, less porosity, and higher precision.28 - 31
This study had the following limitations: a small sample - only 3 laboratories - and a target population not representative of DTs/dentists in Portugal. It should be interpreted as a preliminar study, and future studies must include a larger sample, more laboratories, and other geographic areas to improve knowledge.
It was perceptible that laboratories found it difficult to take the time to answer the questionnaires, and future investigations should be carried out with smaller questionnaires.
Conclusions
Within the limitations of this study, we detected a trend of poor communication between DTs and dentists in Lisbon. The planning and design instructions for RPD construction were insufficient, and the DT designed the RPD componentes in the great majority of cases.
References
1. Ordem dos médicos dentistas (OMD). Barómetro da Saúde Oral 2019. Available from: https://www.omd.pt/observatorio/barometro/barometro2019/. Accessed 20 Feb, 2023.
2. Ordem dos médicos dentistas (OMD). Barómetro da Saúde Oral 2022. Available from:https://www.omd.pt/observatorio/barometro/barometro2022/. Accessed 20 Feb, 2023.
3. Lynch CD, Allen PF. A survey of chrome-cobalt RPD design in Ireland. Int J Prosthodont. 2003;16:362-4.
4. Avrampou M, Kamposiora P, Papavasiliou G, Pissiotis A, Katsoulis J, Doukoudakis A. Design of removable partial dentures: a survey of dental laboratories in Greece. Int J Prosthodont. 2012;25:66-9.
5. Caniço P, Correia A, Campos J. Prótese parcial removível - que informação transmite o médico dentista ao técnico? Rev Port Estomatol Med Dent Cir Maxilofac. 2013;54(S1):e37.
6. Alves Vieira A. Comunicação entre médico dentista e Técnico de Prótese: uma perspetiva laboratorial. Master Thesis. Lisbon: Instituto Superior de Ciências da Saúde Egas Moniz, 2016.
7. Nassani MZ, AlOtaibi MS. Quality of communicating design features for cobalt chromium removable partial dentures in Riyadh, Saudi Arabia. Eur Oral Res. 2020;54:123-9. 168 rev port estomatol med dent cir maxilofac. 2023;64(4):162-169
8. Kumar C, Budhwar P, Shahed S, Syed S, Kolla L, Yasangi M et al. Communication Quality between Prosthodontist and Dental Technician and Its Effects on Prosthetics: An Original Research. Ann Rom Soc Cell Biol. 2021;25:11431-5.
9. EC Medical Devices Directive No 10. Guidelines to Medical Devices Directive 93/42/EEC for Manufacturers of Custom- Made Dental Devices. Dublin: Department of Health and Children, 1997.
10. Rice JA, Lynch CD, McAndrew R, Milward PJ. Tooth preparation for rest seats for cobalt-chromium removable partial dentures completed by general dental practitioners. J Oral Rehabil. 2011;38:72-8.
11Orientações sobre Dispositivos Médicos feitos por medida. Available form: https://www.infarmed.pt/web/infarmed/entidades/dispositivos-medicos/colocacao-no-mercado/orientacoes_dms_medida. Accessed 20 Feb, 2023.
12. Regulamento (UE) 2017/745 do parlamento europeu e do conselho de 5 de abril de 2017. Available form: https://eur-lex.europa.eu/legal-content/PT/TXT/?uri=CELEX%3A32017R0745. Accessed 20 Feb, 2023.
13. Nassar U, Aziz T, Flores-Mir C. Dimensional stability of irreversible hydrocolloid impression materials as a function of pouring time: A systematic review. J Prosthet Dent. 2011;106:126-33.
14. Bilgin MS, Baytaroğlu EN, Erdem A, Dilber E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur J Dent. 2016;10:286-91.
15. Fueki K, Inamochi Y, Wada J, Arai Y, Takaichi A, Murakami N et al. A systematic review of digital removable partial dentures. Part I: Clinical evidence, digital impression, and maxillomandibular relationship record. J Prosthodont Res. 2022;66:40-52.
16. Gan N, Ruan Y, Sun J, Xiong Y, Jiao T. Comparison of Adaptation between the Major Connectors Fabricated from Intraoral Digital Impressions and Extraoral Digital Impressions. Sci Rep. 2018;8:529.
17. Sousa V. Accuracy of intraoral digital impressions and conventional impressions: at the level of partial removable prostheses. Master Thesis. Coimbra: Faculdade de Medicina da Universidade de Coimbra, 2017.
18. Perti S, Vishal Dev S, Kumar Pati S, Mohapatra D. Preference of impression material and technique for complete denture treatment among the dental practitioners in Bhubaneswar: Questionnaire Based Survey. Eur J Mol Clin Med. 2020;7(8):4708-17.
19. Kilfeather G, Lynch C, Sloan A, Youngson C. Quality of communication and master impressions for the fabrication of cobalt chromium removable partial dentures in general dental practice in England, Ireland and Wales in 2009. J Oral Rehabil. 2010;37:300-5.
20. Baig MR, Qudeimat M, Omar R. Assessment of Factors Affecting Partial Removable Dental Prostheses Framework Fit: A Clinical Prospective Study. Int J Prosthodont. 2019;32:497-502.
21. Almortadi N, Chadwick RG. Disinfection of dental impressions – compliance to accepted standards. Br Dent J. 2010;209:607-11.
22. Kugel G, Perry RD, Ferrari M, Lalicata P. Disinfection and Communication Practices: A Survey. J Am Dent Assoc. 2000;131:786-92.
23. Pimentel L, Portugal J, Vasconcelos M, Rocha PA, Sampaio-Fernandes JC. Influência do tratamento térmico na precisão de um silicone de adição autoclavável. Rev Port Estomatol Med Dent Cir Maxilofac. 2014;55:43-8.
24. Pigozzo M, Laganá D, Mori M, Gil C, Mantelli A. Preparos dentais com finalidade protética: uma revisão da literatura. Revista de Odontologia da Universidade Cidade de São Paulo. 2009;21:48-55.
25. Carreiro A, Bezerra C, Amaral B, Piuvezam G, Seabra E. Aspectos Biomecânicos das Próteses Parciais Removíveis e o periodonto de dentes suporte. Periodontia. 2008;18:105-13.
26. Campbell SD, Cooper L, Craddock H, Hyde TP, Nattress B, Pavitt SH et al. Removable partial dentures: The clinical need for innovation. J Prosthet Dent. 2017;118:273-80.
27. Jorge J, Barão V, Delben J, Faverani L, Queiroz T, Assunção W. Titanium in Dentistry:Historical Development, State of the Art and Future Perspectives. J Indian Prosthodont Soc. 2012;13:71-7.
28. Mendes T, Marques D, Lopes L, Caramês J. Total digital workflow in the fabrication of a partial removable dental prostheses: A case report. SAGE Open Med Case Rep. 2019;7:2050313X19871131.
29. Pereira AC, Medeiros AKB, Santos KS, Almeida EO, Barbosa GAS, Carreiro AFP. Accuracy of CAD-CAM systems for removable partial denture framework fabrication: A systematic review. J Prosthet Dent. 2021;125:241-8.
30. Cabrita J, Mendes T, Martins J, Lopes L. Removable partial denture metal framework manufactured by selective laser melting technology – A clinical report. Rev Port Estomatol Med Dent Cir Maxilofac. 2021;62:109-13.
31. Alageel O, Abdallah M, Alsheghri A, Song J, Caron E, Tamimi F. Removable partial denture alloys processed by lasersintering technique. J Biomed Mater Res B App Biomat. 2018;106:1174-85.
Isabel Gomes
E-mail address: isabel.gomes@fmd.ulisboa.pt
CRediT authorship contribution statement
Isabel Gomes: Conceptualization; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Conceptualization; Writing – review & editing. Filipa Reis: Data curation, Investigation, Formal analysis, Visualization, Writing – original draft. Teresa Mendes: Supervision; Visualization; Conceptualization; Writing – review & editing. Luís Miguel Pires Lopes: Visualization; Conceptualization; Writing – review & editing.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interest
The authors have no conflicts of interest to declare.
1646-2890/© 2023 Sociedade Portuguesa de Estomatologia e Medicina Dentária. Published by SPEMD.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).