
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
Revista Portuguesa de Estomatologia Medicina Dentária e Cirurgia Maxilofacial | 2020 | 61 (3) | 148-153
Case report
A diagnostic and clinical approach towards glandular odontogenic cysts: A case report
Uma abordagem diagnóstica e clínica dos cistos odontogênicos glandulares: Relato de caso
a Postgraduate Program in Dental Sciences, Department of Dentistry, Federal University of Rio Grande do Norte, Natal, RN, Brazil
b Oral and Maxillofacial Surgery Residency Program, Department of Dentistry, Federal University of Rio Grande do Norte, Natal, RN, Brazil
Rani I. C. Gonçalo - ranigoncalo@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 61
Issue - 3
Case report
Pages - 148-153
Go to Volume
Article History
Received on 28/01/2020
Accepted on 16/10/2020
Available Online on 03/11/2020
Keywords
Case Report
A diagnostic and clinical approach towards glandular odontogenic cysts: A case report
Uma abordagem diagnóstica e clínica dos cistos odontogênicos glandulares: Relato de caso
Rani I. C. Gonçaloa,*, Carolina M. Camposa, Luiz C. M. Juniorb, Janaina L. M. dos Santosa, Petrus P. Gomesa, Lélia M. G. Queiroza
a Postgraduate Program in Dental Sciences, Department of Dentistry, Federal University of Rio Grande do Norte, Natal, RN, Brazil.
b Oral and Maxillofacial Surgery Residency Program, Department of Dentistry, Federal University of Rio Grande do Norte, Natal, RN, Brazil.
http://doi.org/10.24873/j.rpemd.2020.11.709
Abstract
The glandular odontogenic cyst (GOC) is a rare jaw development cyst that exhibits aggressive biological behavior and is prone to recurrence. The present study aims to report a case of GOC with an emphasis on its clinical, diagnostic, and therapeutic aspects. A 40-year-old female patient presented to the Buccomaxillofacial Surgery service with a swelling in the anterior mandible. Histopathological analysis revealed a cystic cavity lined by a non-keratinized epithelium of varying thickness, exhibiting many features consistent with GOC, such as mucous cells and duct-like microcystic spaces. Lesion resection was performed, followed by immediate reconstruction. After one year of follow-up, the patient is free of recurrence.
Therefore, this case highlights the importance of an effective diagnosis of GOC, through a clear definition of histopathological criteria, to provide the most appropriate treatment and absence of relapses.
Keywords: Diagnosis,Jaw cysts, Mandible,Odontogenic cysts,Treatment
Resumo
O cisto odontogénico glandular (COG) é um cisto de desenvolvimento raro dos ossos maxilares que exibe comportamento biológico agressivo e propensão à recorrência. O objectivo do presente estudo é relatar um caso de COG com ênfase em seus aspectos clínicos, diagnósticos e terapêuticos. Paciente do sexo feminino, 40 anos, compareceu ao serviço de Cirurgia Bucomaxilofacial apresentando aumento de volume na região anterior de mandíbula.
A análise histopatológica revelou a presença de uma cavidade cística revestida por um epitélio não queratinizado de espessura variável, exibindo características consistentes com COG, como células mucosas e espaços microcísticos semelhantes a ductos. Foi realizada ressecção da lesão, seguida de reconstrução imediata. Após um ano de acompanhamento, a paciente encontra-se livre de recorrências. Dessa forma, este caso destaca a importância de um diagnóstico eficaz de COG, através da definição clara dos critérios histopatológicos, a fim de proporcionar o tratamento mais adequado e a ausência de recidivas.
Palavras-chave: Diagnóstico, Cistos maxilares,Mandíbula,Cistos odontogénicos,Tratamento.
Introduction
The glandular odontogenic cyst (GOC) is a rare jaw development cyst. It was initially described by Padayachee and Van Wyk1 as a “sialo‑odontogenic cyst” due to the presence of glandular elements,2 and only in the following year when eight cases of this same lesion were reported, its currently used term was proposed.3, 4 In 1992, the World Health Organization (WHO) included GOC in its classification, describing it as “a cyst that originates in the dental support areas of the jawbones and is characterized by an epithelial lining with columnar or cuboidal cells, either on the surface or in its lining, with crypts or cyst‑like spaces within the epithelium thickness.”5, 6 The last edition of the WHO Classification of Head and Neck Tumors, published in 2017, defines GOC as a development cyst with epithelial characteristics that simulate the salivary gland or glandular differentiation.7
On clinical examination, GOC presents as an asymptomatic slow‑growing swelling, affecting most commonly the anterior mandible region. It usually affects individuals between the 5th and 7th decades of life,2 with a slight predilection for males. Radiographic examinations reveal a radiolucent unilateral or multilocular intraosseous lesion with well‑defined margins, which may show cortical perforation and tooth displacement. However, clinical and radiographic characteristics are non‑specific and may mimic other destructive damage to the jawbones. Therefore, performing a biopsy is of great clinical importance to obtain a proper diagnosis and, consequently, begin treatment.8
Since GOCs are characterized by aggressive biological behavior and a high recurrence rate, the therapeutic approach is quite controversial, ranging from enucleation and curettage to en bloc resection, with the possibility of bone graft for immediate reconstruction.9 Therefore, the present study aims to present a clinical case of GOC with an emphasis on its clinical‑pathological characteristics, diagnosis, and clinical management.
Case report
A 40‑year‑old black female patient attended the Buccomaxilofacial Surgery and Traumatology service of the Federal University of Rio Grande do Norte (Natal, RN, Brazil), with the chief complaint of painless swelling of the jaw for 6 months (Figure 1). Intraoral examination revealed a bluish‑colored swelling of the anterior mandible with a hardened consistency and approximately 4 cm in diameter, in the region of teeth 3.1, 3.2, and 3.3, which responded positively to the vitality test (Figure 2).

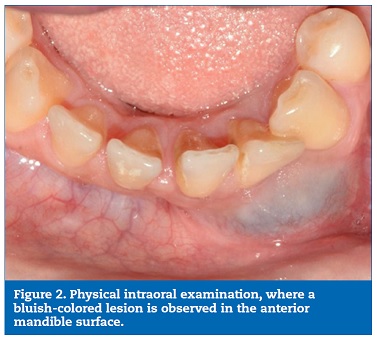
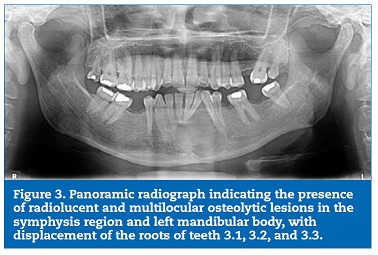
Mobility and increased periodontal probing depth were not observed. A panoramic radiograph revealed radiolucent and multilocular lesions associated with tooth displacement (Figure 3).
The patient was initially submitted to an aspiration puncture in the lesion, which confirmed its cystic nature. Then, we performed an incisional biopsy in the more exteriorized region of the lesion, evidenced by the bluish color in the mucosa. The dimensions of the tissue fragment removed were 3.3 x 2.0 x 0.3 cm. Odontogenic keratocyst and botryoid odontogenic cyst were considered as diagnostic hypotheses.
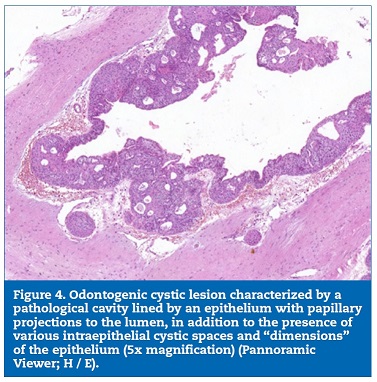
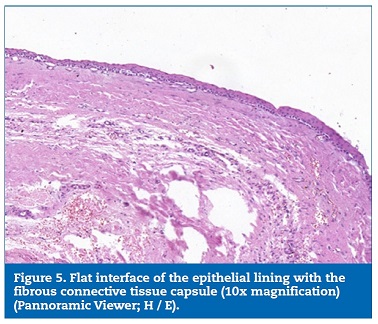
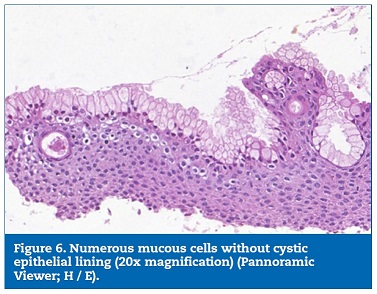
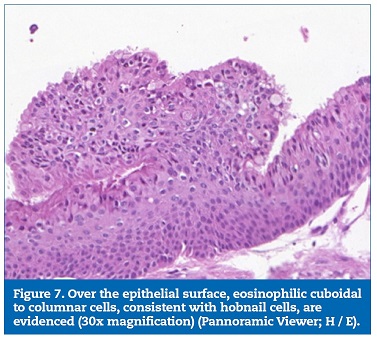
A histopathological examination revealed a pathological cavity lined with a non‑keratinized stratified squamous epithelium of varying thickness, with columnar and sometimes ciliated cells. Mucous cells and duct‑like microcystic spaces containing amorphous, mucus‑compatible eosinophilic material were also evidenced. Moreover, eosinophilic cuboidal or columnar cells (hobnail cells) were evidenced on the epithelir al lining surface. The capsule, composed of dense fibrous connective tissue, was adjacent to the cystic epithelium (Figures 4, 5, 6, 7). Thus, based on the clinical and microscopic findings, the histopathological diagnosis was GOC.
Due to GOC’s high recurrence rate, the surgical plan consisted of lesion resection followed by immediate reconstruction.
A multi‑slice computed tomography was then requested for a detailed evaluation of the lesion and development of a prototype biomodel. Preoperative laboratory tests and surgical risk assessment were also requested.
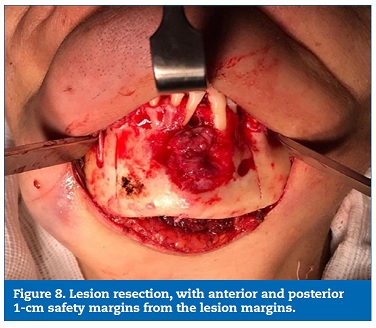
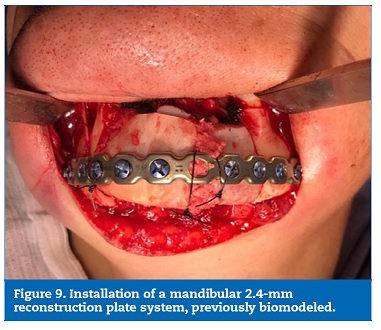
The lesion was resected with a safety margin (0.5 cm), generating a 4‑cm defect in the mandibular segment, followed by the fitting of a mandibular reconstruction plate (Figures 8, 9, 10).

Simultaneously, the medical team performed graft removal from the anterior iliac crest region, thus enabling subsequent preparation, adaptation, and fixation of the graft in the resected area, using 2.4‑mm system screws. Finally, muscle resuspension was performed on the plate, followed by access suture and compressive dressing application. The patient was under general anesthesia during the surgery. Prophylactic medication consisting of intravenous cephalothin (1 g), dexamethasone (10 mg), and dipyrone (1 g) was administered and maintained in the postoperative period with adequate doses. During the immediate postoperative period, the patient had no pain complaints and presented with edema compatible with the performed procedure and limited mouth opening.
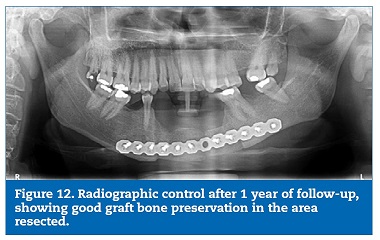
The histopathological diagnosis was confirmed by the excisional biopsy, with free lesion margins. The patient has been under follow‑ up for 1 year, with no recurrences at the moment and good graft bone preservation (Figures 11 and 12).

Discussion and conclusions
This article highlights clinical, diagnostical, and therapeutic GOC aspects. Due to its aggressive biological behavior and high recurrence rate, studies and case reports that describe its occurrence are of significant clinical relevance, contributing to proper diagnosis and clinical management, as well as providing a broad view of the surgical techniques that may be adopted.
With an estimated prevalence of 0.17% of all gnathic cysts,10 GOC is a rare but relatively well‑known entity with well‑described microscopic characteristics. Clinically, GOC tends to affect most commonly the mandible, especially its anterior region, followed by the anterior maxilla.11 In most cases, cortical expansion is observed, with or without cortical perforation, as well as root resorption and tooth displacement, which indicate the aggressiveness potential of this type of lesion.8 Despite presenting non‑specific radiographic characteristics, most cases present as multilocular lesions.11 In the present report, the anterior mandible had a radiolucent and multilocular radiographic appearance associated with radicular dislocation.
Regarding histopathological aspects, microscopic characteristics are categorized into major and minor criteria.12 Major criteria must be present for diagnosis, while smaller criteria are favorable for diagnosis but not mandatory.13 However, there is still no consensus on how many criteria would be required for the diagnosis. In a multicenter retrospective study, all cases analyzed exhibited eosinophilic cuboid cells (hobnail), a non‑specific feature required for GOC diagnosis. In addition, those authors reported that some of the most useful microscopic features that distinguish GOC from other lesions that may mimic it are [1] microcysts; [2] epithelial spheres; [3] clear cells; [4] variable thickness of the epithelial cyst lining; and [5] multiple compartments.2 Thus, the present case is highly predictive of GOC, as all aforementioned characteristics were present, in addition to the presence of ciliate and mucous cells.
GOC may exhibit morphological similarities to other cystic jaw lesions, such as dentigerous cysts displaying metaplastic changes, ciliated surgical cysts, lateral periodontal cysts, root cysts, residual cysts with mucous metaplasia, and botryoid odontogenic cysts.2, 8 The low‑grade variant of the central mucoepidermoid carcinoma should also be considered a differential GOC diagnosis since these lesions share certain histopathological features, such as the presence of clear and mucous cells and mucin‑filled cystic spaces.7, 11 In addition, in rare cases, GOC may contain small islands in the cystic wall that resemble mucoepidermoid carcinoma. This microscopic aspect suggests that GOC and central mucoepidermoid carcinoma may share a histopathological spectrum, although it is unknown whether this finding is associated with more aggressive or malignant behavior.2
Histochemical and immunohistochemical techniques may be used as adjunctive tools to histological and morphological features to obtain an accurate diagnosis. Special stains, such as mucicarmine and periodic acid‑Schiff (PAS), are used to confirm the presence of mucin in the lesion. Also, immunohistochemical staining with cytokeratin 19 (CK19) reveals strong, homogeneous positivity in all the epithelium layers, which confirms its odontogenic nature.11, 14 The expression of cytokeratins has been reported to differ between GOCs and central mucoepidermoid carcinoma, suggesting that CK18 and CK19 could help distinguish these two entities.15
As is well‑known, GOC exhibits an unpredictable and aggressive clinical behavior associated with a high incidence of cortical perforation and a relatively high recurrence rate, directly related to lesion size.4, 11 The literature reports a preference for more conservative therapeutic approaches, such as enucleation, curettage, excision, cystectomy, and peripheral ostectomy.2, 8 However, a study showed that cases treated by radical surgical procedures did not recur, while 35.9% of conservatively treated cases did.8 Enucleation and curettage are most associated with a higher risk of recurrence, especially in large and multilocular lesions. In these situations, it is preferable to adopt more aggressive therapeutic measures, in addition to long‑term patient follow‑up.
The use of adjuvant methods such as peripheral osteotomy or marginal resection is associated with a significant reduction in lesion recurrence.8, 11, 12 In the present case, a more radical therapeutic approach was adopted with segmental resection followed by immediate reconstruction to reduce the lesion recurrence risks. After one year of lesion excision, the patient has no signs of relapse. Nevertheless, a long‑term follow‑up of the patient is still required to keep up with a possible recurrence.
Due to its rarity, performing controlled studies comparing different GOC therapeutic approaches is difficult. A clear definition of histopathological criteria is essential to aid with the diagnosis, as well as searches for specific markers that support the diagnosis. Histochemical (mucicarmine and PAS) and immunohistochemical (CK‑19) techniques may be useful tools to verify unclear cases, especially to differentiate from central mucoepidermoid carcinoma. Thus, greater diagnostic accuracy contributes to the adoption of appropriate personalized therapeutic measures.
References
1. Padayachee A, Van Wyk CW. Two cystic lesions with features of both the botryoid odontogenic cyst and the central mucoepidermoid tumour: Sialo‑odontogenic cyst? J Oral Pathol. 1987;16:499–504.
2. Fowler CB, Brannon RB, Kessler HP, Castle JT, Kahn MA. Glandular odontogenic cyst: Analysis of 46 cases with special emphasis on microscopic criteria for diagnosis. Head Neck Pathol. 2011;5:364–75.
3. Gardner DG, Kessler HP, Morency R, Schaffner DL. The glandular odontogenic cyst: An apparent entity. J Oral Pathol. 1988;17:359–66.
4. Purohit S, Shah V, Bhakhar V, Harsh A. Glandular odontogenic cyst in maxilla: A case report and literature review. J Oral Maxillofac Pathol. 2014;18:320‑3.
5. Kramer IR, Pindborg JJ, Shear M. The WHO histological typing of odontogenic tumours. A commentary on the second edition. Cancer. 1992;70:2988–94.
6. Gurler G, Al‑Ghamian H, Aksakalli N, Delilbasi C. Glandular odontogenic cyst: Case Series. Contemp Clin Dent. 2017;8:653–7.
7. EI‑Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. WHO Classification of Head and Neck Tumours. 4th ed. Lyon:IARC; 2017.
8. Kaplan I, Anavi Y, Hirshberg A. Glandular odontogenic cyst: A challenge in diagnosis and treatment. Oral Dis. 2008;14:575‑81.
9. Momeni Roochi M, Tavakoli I, Ghazi FM, Tavakoli A. Case series and review of glandular odontogenic cyst with emphasis on treatment modalities. J Craniomaxillofac Surg. 2015;43:746‑50.
10. Krishnamurthy A, Sherlin HJ, Ramalingam K, Natesan A, Premkumar P, Ramani P, et al. Glandular odontogenic cyst: Report of two cases and review of literature. Head Neck Pathol. 2009;3:153‑8.
11. Urs AB, Kumar P, Augustine J, Malhotra R. Glandular odontogenic cyst: Series of five cases. J Oral Maxillofac Pathol. 2017;21:239–43.
12. Kaplan I, Gal G, Anavi Y, Manor R, Calderon S. Glandular odontogenic cyst: Treatment and recurrence. J Oral Maxillofac Surg. 2005;63:435‑41.
13. Tavargeri AK, Anehosur V, Niranjan KC, Nayyar A. Case report of a rare glandular odontogenic cyst in a child: A diagnostic dilemma. Int J Health Sci (Qassim). 2019;13:53–5.
14. Mascitti M, Santarelli A, Sabatucci A, Procaccini M, Lo Muzio L, Zizzi A, et al. Glandular odontogenic cyst: review of literature and report of a new case with cytokeratin‑19 expression. Open Dent J. 2014;8:1‑12.
15. Pires FR, Chen SY, da Cruz Perez DE, de Almeida OP, Kowalski LP. Cytokeratin expression in central mucoepidermoid carcinoma and glandular odontogenic cyst. Oral Oncol. 2004;40:545‑51.
Rani Iani Costa Gonçalo
E-mail address: ranigoncalo@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed their work center protocols on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interest
The authors have no conflicts of interest to declare.
Acknowledgment
This study was partially financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil – Finance Code 001.
Article history:
Received 28 January 2020
Accepted 16 October 2020
Available online 3 November 2020