
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD | 2019 | 60 (4) | 197-204
Case report
Endodontic management of maxillary permanent first molar with seven root canals – Report of two cases
Tratamento endodôntico de molar superior com 7 canais radiculares – relato de dois casos
a Department of Endodontics, Faculdade de Medicina Dentária, Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
b Centro de Estudo de Medicina Dentária Baseada na Evidência, Faculdade de Medicina Dentária, Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
c Unidade de Investigação em Ciência Orais e Biomédicas, Faculdade de Medicina Dentária (UICOB-FMDUL), Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
Mariana Domingos Pires - mariana.dpires@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 60
Issue - 4
Case report
Pages - 197-204
Go to Volume
Article History
Received on 22/10/2019
Accepted on 10/12/2019
Available Online on 10/12/2019
Keywords
Case report
Endodontic management of maxillary permanent first molar with seven root canals – Report of two cases
Tratamento endodôntico de molar superior com 7 canais radiculares – relato de dois casos
Mariana Domingos Pires a,*, Jorge N.R. Martinsa,b,c
a Department of Endodontics, Faculdade de Medicina Dentaria, Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
b Centro de Estudo de Medicina Dentaria Baseada na Evidencia, Faculdade de Medicina Dentaria, Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
c Unidade de Investigacao em Ciencia Orais e Biomedicas, Faculdade de Medicina Dentaria (UICOB-FMDUL), Universidade de Lisboa (University of Lisbon), Lisbon, Portugal
http://doi.org/10.24873/j.rpemd.2020.01.692
Abstract
The maxillary first molar has been presented as a tooth with an enormous variety of root canal system configurations. The purpose of this paper is to present two cases of maxillary first molars displaying an uncommon seven root canal system morphology. After a proper access opening of the maxillary molars undergoing a root canal treatment, two dark developmental grooves were seen connecting both the main buccal canals to the palatal one.
Under the magnification and illumination of a dental operating microscope, these two grooves were explored with ultrasonic tips, which allowed identifying several other root canal orifices in both buccal roots complemented by a single palatal root canal in one case, and two in the other. Embryological reasons and the best clinical approaches to these complex morphologies are also debated. Bearing in mind the complexities of internal anatomy can help maximize the success rates of endodontic treatment.
Keywords: Anatomy, Endodontics,Molar, Morphology,Root canal therapy
Resumo
O primeiro molar superior definitivo é descrito com uma enorme variedade de configurações do sistema canalar. Neste trabalho apresentamos dois casos de molares superiores com uma morfologia invulgar de 7 canais radiculares. Depois de estabelecido o acesso à câmara pulpar, foram detetados dois sulcos de desenvolvimento com coloração mais escura a interligar os dois canais vestibulares principais ao palatino. Sob ampliação e iluminação do microscópio cirúrgico, estes dois sulcos foram explorados com pontas ultrassónicas, o que permitiu identificar vários orifícios de entrada canalar adicionais em ambas as raízes vestibulares complementadas por um único canal palatino num dos casos, e dois no outro. Debatemos também as questões de desenvolvimento embrionário relacionadas com as diferentes configurações anatómicas e as melhores abordagens clínicas para estes casos. Reconhecer as complexidades da anatomia interna canalar pode contribuir para maximizar a taxa de sucesso do tratamento endodôntico
Palavras-chave: Anatomia,Endodontia,Molar, Morfologia, Tratamento endodôntico
Introduction
The morphology of the maxillary first molar has been extensively studied over the years. The most common pulp chamber floor configuration for the maxillary first molar is the presence of four root canal orifices,1 but configurations ranging from one to eight root canals have also been reported.1-3 Root fusion with main root canals merging4 or even C-shaped anatomies (5) have also been documented.
The scientific evidence shows that the clinical efficacy of root canal therapy is not only associated with correct coronary rehabilitation but is also clearly linked with complete instrumentation, disinfection and obturation of the root canal system.6 The preoperative periapical status has also been pointed out as a potential prognostic factor for the success of both primary and secondary non-surgical root canal treatment.7 Moreover, even under controlled conditions, persistent periapical inflammation may develop, or persist, as a tissue response to the endodontic treatment.8The anatomic variation of the maxillary first molar is wide, and, although understanding the anatomy of the tooth under treatment may be a challenge, it is unarguably important. Several authors have stated that previous root canal treatment failures might be associated with endodontic therapies that leave missed and untreated root canals.9, 10
The objective of this paper is to present two cases of an uncommon configuration of the maxillary first molar presenting three roots and seven root canals.
Case reports
Case # 1
A 52-year-old Caucasian female was referred to an emergency appointment with a chief complaint of spontaneous and acute pain in the maxillary left side, which tended to increase with cold temperature. The reported medical history was non-contributory. On clinical examination, a large carious lesion was observed on the mesial and occlusal aspects of the maxillary left first molar (tooth 26); however, no periodontal pockets were noted, the tooth mobility was within physiological limits and none of the teeth 25, 26 or 27 were tender to percussion or palpation. The response to the cold-sensitive test (Endo cold spray, Henry Schein, Germany) was an intense pain on tooth 26 and normal response on tooth 27. The preoperative radiographic examination confirmed the involvement of tooth 26 (Figure 1).

Considering the clinical and radiographic findings, tooth 26 was diagnosed with symptomatic irreversible pulpitis with normal periapical tissues. Root canal treatment was scheduled after being accepted by the patient.
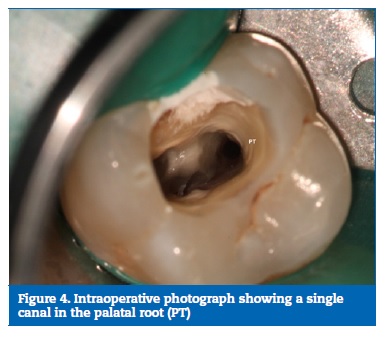
Following a buccal infiltration anesthesia performed using 1.8 mL of 4% articaine with 1:200.000 epinephrine (Artinibsa, Inibsa, Spain), proper rubber dam (R&S Dental Dam, CFPM, France) isolation was obtained. The carious lesion was excavated, and the endodontic access prepared. A careful inspection of the pulp chamber floor was possible after the removal of loose pulp stones with the aid of a #2 ProUltra ultrasonic tip (ProUltra, Dentsply Maillefer, USA). Three main root canal orifices were identified: mesiobuccal (MB1), distobuccal (DB1) and palatal (P). Upon a more detailed observation of the chamber floor using a surgical microscope (Opmi Pico, Carl Zeiss Surgical, Germany), two dark developmental grooves were observed connecting both the main buccal canals to the palatal one.
These developmental grooves were explored with #2 ProUltra ultrasonic tip troughing, and four extra canals were detected (MB2, MB3, DB2 and DB3). A total of seven root canals were identified (Figures 2, 3, 4).


All canals were negotiated using an ISO size.08 stainless-steel hand file, and the working length was determined by an electronic method using a Root Zx II locator (Root Zx II, Morita, USA) and confirmed radiographically. Coronal flaring was performed with a ProTaper SX rotary file (ProTaper Universal, Dentsply Maillefer, Switzerland) and hand instrumentation until an ISO size.15 stainless-steel hand file could reach the previously established working length in order to obtain a manual glide path. The mechanical instrumentation was performed following the ProTaper Universal sequence with S1, S2 and F1 rotary files (ProTaper Universal, Dentsply Maillefer, Switzerland), as recommended by the manufacturer. The palatal root canal was the only one finished at an F2 file. An endodontic rotary motor (Dentaport ZX, J.Morita, Japan) was used to accomplish the mechanical debridement, using medium torque and 300 rotations per minute. The mechanical debridement was accomplished under continuous intracanal irrigation with 5.25% sodium hypochlorite (Denta Flux, J. Ripoll SL, Spain) at room temperature.
The treatment was planned for two appointments due to time limitations related to the technical procedures of the first visit. To prevent further coronal microleakage between appointments, a dressing of calcium hydroxide (Ultracal, Ultradent, USA) was placed with a lentulo as intracanal medication, and the access cavity was provisionally restored with IRM filling (IRM, Dentsply, Germany).
At the time of the second appointment, two weeks later the tooth under treatment was asymptomatic. After buccal anesthesia, rubber dam isolation and removal of the temporary restoration, the calcium hydroxide dressing was washed out with continuous irrigation with 5.25% sodium hypochlorite.
The cleanliness of the root canals was verified with a surgical microscope. The final irrigation protocol included one-minute irrigation with 17% EDTA (EDTA, Laboratorios Clarben S.A., Spain), followed by a final flush with 5.25% sodium hypochlorite and alcohol rinses. Paper points were used to dry the root canals, which were posteriorly filled with gutta-percha and AH Plus sealer (AH Plus, Dentsply, Germany) using the continuous wave condensation technique (Figures 5, 6). A System B unit (System B, Sybron Endo, USA) was used for downpacking and an Obtura II unit (Obtura II, Obtura Spartan, USA) was used for backfilling. After root canal filling procedures, the pulp chamber was cleaned with alcohol, the entrance of the root canals orifices was closed with a flowable composite resin (Supraflow, R&S, CFPM, France) and the access cavity was temporarily restored. The patient was scheduled for definitive coronal rehabilitation (Figure 7). The 15-month recall showed no clinic or radiographic findings (Figure 8).




Case # 2
A 38-year-old Caucasian male reporting a non-contributory previous medical history attended an emergency appointment with a chief complaint of spontaneous and increased pain with cold in the maxillary right side. A careful clinical and radiographic observation , which was performed using a recent panoramic radiograph avoiding unnecessary radiation exposure of a supplemental preoperative x-ray, following the ALARA principles,11 revealed a large carious lesion on the mesial and distal aspects of the maxillary right first molar (tooth 16) (Figure 9).

No periodontal pockets were noted, and the tooth mobility was within healthy limits. Teeth 15, 16 and 17 were not tender to palpation or percussion. The response to the cold-sensitive test (Endo cold spray, Henry Schein, Germany) was an intense pain on tooth 16 and normal response on tooth 17. A diagnosis of irreversible pulpitis with normal apical tissues on tooth 16 was established. The case was scheduled for root canal treatment after being accepted by the patient.
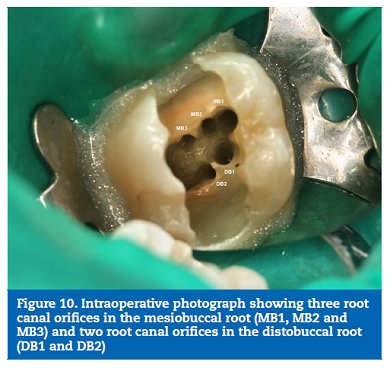
The treatment protocol was similar to the one detailed for Case #1, except for the instrumentation sequence, which was done with the Protaper Next rotary system up to X2 in all canals (Dentsply Maillefer, Switzerland). In this case, the root canal therapy was completed in a single session. The distribution of the seven canals – MB1, MB2, MB3, DB1, DB2, PT1, PT2 (Figures 10, 11, 12, 13 and 14) – also differed from the previous case. One year after treatment, the patient was contacted for a follow-up appointment, but he declined and added that the tooth was in function and asymptomatic.




Discussion and conclusions
The root development starts after the crown formation is completed. Epithelial cells of the inner and outer dental epithelium meet in the apical end at a junction named cervical loop, forming the Hertwig’s horizontal root sheath or horizontal diaphragm. The apical end of the horizontal diaphragm bends to form a collar-like structure. In the single-rooted teeth, the horizontal diaphragm grows like a tube around the newly formed pulp. In the multi-rooted teeth, epithelial cells from the horizontal diaphragm develop extensions that grow toward the center until they contact each other, dividing the original single diaphragm into several horizontal diaphragms, one for each root.12
Prior to root formation, at the late bell stage of tooth development, the most peripheral cells of the dental papilla differentiate into odontoblasts, which are responsible for the dentin matrix secretion in a process called dentinogenesis.
The primary and secondary dentinogenesis are responsible for the formation of the root canal system. The primary dentin is formed at a fast pace prior to the tooth eruption, while the secondary dentin is formed at a very slow pace all around the internal periphery of the crown and roots, after the tooth eruption and during the lifetime.13 This leads to dentin matrix deposition on the floor and roof of the pulp chamber and inside the root canals which, in turn, leads to pulp recession and the formation of complex root canals systems.
There is an intimate relationship between angiogenesis and dentinogenesis.13 The microcirculatory system of the pulp is composed of arterioles, the largest vessels of the pulp, which end in the capillary layers that reach as far as the sub-odontoblastic region. The thin wall of a capillary works as a semipermeable membrane that allows the exchange of substances, including nutrients that will allow the correct function of the odontoblast cells during dentinogenesis.
Because of this strong correlation between blood supply and tooth development, the deposition of dentin matrix takes place near blood vessels, and the capillary layers must reach all the pulp cells.14 This may justify the presence of complex root canals systems with more than one root canal and the isthmus between these canals in a single very large root, as is the case of the mesiobuccal root of the maxillary molar. Larger roots need a larger and more complex microcirculatory system, which may lead to a more complex dentin matrix deposition around this circulatory system, resulting in more complex root canal anatomies that potentially increase the endodontic procedures’ difficulty.
This dentinogenesis may lead to different anatomic configurations of the maxillary first molar. Several of them have been already reported in the scientific literature. The review by Cleghorn et al.1 makes an extensive analysis of the data available on the anatomy of the first upper molar. Regarding the mesiobuccal root, in an overall sample of 8399 roots from 34 ex vivo and in vivo studies, one root canal (MB) was identified in 43.1% of the cases and two root canals (MB1 and MB2) in 56.8%. The distobuccal root review had an overall sample of 2576 roots from 14 laboratory and clinical studies. The incidence of a single canal (DB) was 98.3% and the presence of two canals (DB1 and DB2) was found in 1.7% of the cases. Only a few reports3, 15 described three root canals in the MB root, and this may be found in the DB root very rarely. In this report, two seven root canal configurations – a rare configuration with scarce reports available, are presented.1, 15 In the present cases, three canals were found in both mesiobuccal and distobuccal roots. The mesiobuccal roots had a Gulabivala type 2 (3-2) configuration in both cases, the distobuccal had a Gulabivala type 1 (3-1) configuration in Case #1 and a Vertucci type II (2-1) in Case #2, while the palatal root had a Vertucci type I (1-1) in Case #1 and type V (1-2) in Case #2.16
As for the techniques used to approach these cases clinically, some aspects should be considered. A correct diagnosis of the anatomy is important. The surgical microscope works as a valuable tool when exploring the pulp chamber floor,17, 18 allowing to detect all the depressions and isthmuses that may hide root canal orifices. Exploring those depressions and isthmuses with ultrasonic troughing is highly effective.19 In addition to periapical radiographs, the cone-beam computed tomography (CBCT) might be useful for the assessment and appreciation of extremely complex root canal systems prior to, and aiming to enhance, endodontic management.20
Technically, the over-enlargement of the root canals should be avoided at all costs in cases with multiple canal configurations, to minimize the chance of root weakness. To overcome the challenges of the isthmus and root canal system irregularities, thermoplastic obturation techniques should be preferred.21 The agitation of ultrasonic irrigation has been documented as capable of improving irrigation effects and may be very useful for these configurations full of complexities.22
References
1. Cleghorn BM, Christie WH, Dong C. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod. 2006;32:813-21.
2. Gopikrishna V, Bhargavi N, Kandaswamy D. Endodontic management of a maxillary first molar with a single root and a single canal diagnosed with the aid of spiral CT: a case report. J Endod. 2006;32:687-91.
3. Kottoor J, Velmurugan N, Surendram S. Endodontic management of a maxillary first molar with eight root canal system evaluated using cone-beam computer tomography scanning: a case report. J Endod. 2011;37:715-9.
4. Zheng Q, Wang Y, Zhou X, Wang Q, Zheng G, Huang D. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36:1480-4.
5. Newton CW, McDonald S. A C-shaped canal configuration in a maxillary first molar. J Endod. 1984;10:397-9.
6. Friedman S. Prognosis of initial endodontic therapy. Endod Topics. 2002;2:59-88.
7. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011;44:583-609.
8. Santos JM, Palma PJ, Ramos JC, Cabrita AS, Friedman S. Periapical inflammation subsequent to coronal inoculation of dog teeth root filled with resilon/epiphany in 1 or 2 treatment sessions with chlorhexidine medication. J Endod. 2014;40:837-41.
9. Baruwa AO, Martins JNR, Meirinhos J, Pereira B, Gouveia J, Quaresma SA, Monroe A, Ginjeira A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J Endod. 2019:in press.
10. Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S, Meyers J. A 5 yr clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2005;31:262-4.
11. AAE and AAOMR joint position statement: use of cone beam computed tomography in Endodontics 2015 update. J Endod 2015;41:1393-6.
12. Castellucci A. Embriology. In: Castellucci A. Endodontics Vol. I. 1st ed. Florence, ITA: Il Tridente, 2004:6-23.
13. Smith AJ. Dentin formation and repair. In: Haegreaves K, Goodis H. Seltzer and Bender´s dental pulp, 3rd ed. Hanover Park, IL, USA: Quintessence Publishing Co, Inc., 2002:41-62.
14. Suda H, Ikeda H. The circulation of the pulp. In: Haegreaves K, Goodis H. Seltzer and Bender´s dental pulp, 3rd ed. Hanover Park, IL, USA: Quintessence Publishing Co, Inc., 2002:123-150.
15. Baratto-Filho F, Zaitter S, Haragushiku G, Campos E, Abuabara A, Correr G. Analysis of the internal anatomy of maxillary first molars by using different methods. J Endod. 2009;35:337-42.
16. Gutmann JL, Fan B. Tooth Morphology, Isolation, and Access. In: Haegreaves K, Berman LH. Cohen’s Pathways of the Pulp, 11th edi. Saint Louis, MO, USA: Elsevier Inc, 2016:137-138
17. Mamoun JS. The maxillary molar endodontic access opening: A microscope based approach. Eur J Dent. 2016;10:439-46.
18. Tuncer A, Haznedaroglu F, Sert S. The location and accessibility of the second mesiobuccal canal in maxillary first molar. Eur J Dent. 2010;4:12-6.
19. Weller RN, Hartwell GR. The impact of improved access and searching techniques on detection of the mesiolingual canal in maxillary molars. J Endod. 1989;15:82-3.
20. Patel S, Brown J, Semper M, Abella F, Mannocci F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE). Int Endod J. 2019;52:1675-8.
21. Lea C, Apicella M, Mines P, Yancich P, Parker M. Comparison of the obturation density of cold lateral compaction versus warm vertical compaction using the continuous wave of condensation technique. J Endod. 2005;31:37-9.
22. Virdee SS, Seymour DW, Farnell D, Bhamra G, Bhakta S. Efficacy of irrigant activation techniques in removing intracanal smear layer and debris from mature permanent teeth: a systematic review and meta-analysis. Int Endod J. 2018;51:605-21.
Mariana Domingos Pires
E-mail address: mariana.dpires@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interest
The authors have no conflicts of interest to declare.
Article history:
Received 22 October 2019
Accepted 10 December 2019
Available online 7 January 2020