
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
Rev Port Estomatol Med Dent Cir Maxilofac | 2017 | 58 (1) | 17-22
Original research
Microleakage of different root canal sealers in absence of a coronal restorative material
Microinfiltração de diferentes cimentos obturadores na ausência de um material restaurador coronário
a School of Dentistry, Federal University of Amazonas, Manaus, AM, Brazil
b Superior School of Health Sciences, State University of Amazonas, Manaus, AM, Brazil
c Department of Dentistry - Endodontics Division, Health Sciences Center, Federal University of Santa Catarina, Florianópolis, SC, Brazil
Lucas da Fonseca Roberti Garcia - drlucas.garcia@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 58
Issue - 1
Original research
Pages - 17-22
Go to Volume
Article History
Received on 11/09/2016
Accepted on 27/12/2016
Available Online on 31/03/2017
Keywords
Original research
Microleakage of different root canal sealers in absence of a coronal restorative
material
Microinfiltração de diferentes cimentos
obturadores na ausência de um material restaurador coronário
Izabelly Esteves Bittencourt Martinsa, Mariana Menna Barreto Bastosa, Angela Delfina Bitencourt Garridoa, André Augusto Franco Marquesb, Lucas da Fonseca Roberti Garciac,*, Emílio Carlos Sponchiado Júniora
aSchool of Dentistry, Federal University of Amazonas, Manaus, AM, Brazil. bSuperior School of Health Sciences, State University of Amazonas, Manaus, AM, Brazil. cDepartment of Dentistry – Endodontics Division, Health Sciences Center, Federal University of Santa Catarina, Florianópolis, SC, Brazil.
http://doi.org/10.24873/j.rpemd.2017.05.007
Abstract
Objectives: The aim of this study was to evaluate the level of coronal microleakage in root canals filled with MTA Fillapex, in comparison with two root canal sealers of different bases, Sealapex and AH Plus.
Methods: Sixty-six mandibular premolars were prepared and randomly distributed into three groups, according to the root canal sealer used for filling, as follows: G1 AH Plus (Dentsply-Maillefer), G2 MTA Fillapex (Ângelus) and Sealapex (Kerr Corporation). After one week in an oven (37°C, 100% humidity), the teeth were immersed in India ink for 15 and 30 days (n = 10), and then submitted to diaphanization to verify the amount of coronal microleakage using an operating microscope. The values were statistically analyzed using Kruskal-Wallis test (p < 0.05).
Results: MTA Fillapex had the highest coronal microleakage values, in both periods (15 and 30 days). Coronal microleakage mean values were only significant in comparison with AH Plus group at the 15 day-period (p < 0.05).
Conclusions: None of the tested cements was able to prevent coronal microleakage. However, MTA Fillapex had the worst results at 15 days.
Keywords: Coronal leakage, Endodontics, Root canal filling material
Resumo
Objetivos:O objetivo deste estudo foi avaliar o nível de infiltração coronal em canais radiculares obturados com MTA Fillapex, em comparação a dois cimentos endodônticos de diferentes bases, Sealapex e AH Plus.
Métodos: Sessenta e seis pré-molares inferiores foram preparados e distribuídos aleatoriamente em três grupos, de acordo com o cimento endodôntico utilizados para obturação, da seguinte maneira: G1 AH Plus (Dentsply-Maillefer), G2 MTA Fillapex (Ângelus) e Sealapex (Kerr Corporation). Depois de uma semana em estufa (37°C, 100% de humidade relativa), os dentes foram imersos em corante durante 15 e 30 dias (n = 10), e em seguida, submetidos a diafanização para verificar a quantidade de infiltração coronária utilizando microscópio operatório. Os valores foram analisados estatisticamente pelo teste de Kruskal-Wallis (p < 0,05).
Resultados: MTA Fillapex apresentou os maiores valores de microinfiltração, em ambos os períodos (15 e 30 dias). Os valores médios de microinfiltração coronal foram significativos apenas em comparação ao grupo AH Plus grupo no período de 15 dias (p < 0,05).
Conclusões: Nenhum dos cimentos testados foi capaz de evitar a microinfiltração coronária. No entanto, MTA Fillapex teve os piores resultados aos 15 dias de análise.
Palavras-chave: Infiltração coronária, Endodontia, Material obturador
Introduction
After proper cleaning and shaping, the root canal system must be three-dimensionally filled with materials that ensure its impervious seal, preventing marginal leakage, and creating a favorable environment for biological repair of periapical tissues.1
As gutta-percha has no adhesion to dentin surface, the choice of sealers that allow adhesion between gutta-percha and dental structure, and have relative bioactivity, assisting in the repair process, are fundamental.2,3
Over the years, the development of several biomaterials enabled the professional to solve a large number of cases in endodontic practice.4 Among these biomaterials, Mineral Trioxide Aggregate (MTA) has been widely used due to its excellent biological properties,4-6 despite some negative features, as poor handling carachteristics, long setting-time and low flow ability.3,4
In order to incorporate the biological properties of MTA to a material with proper handling carachteristics and adequate sealing, a new root canal sealer, called MTA Fillapex (Ângelus, Londrina, PR, Brazil), was developed. MTA Fillapex is a mineral aggregate-based root canal sealer, which comprises particles of MTA – dicalcium and tricalcium silicate – (13%) (wt), salicylate resin, nanoparticulated silica and bismuth trioxide as radiopacifier agent.7 According to the manufacturer, such sealer mixes the excellent biological features of MTA to the sealing ability of modern resin-based root canal sealers. Studies have reported that this sealer is biocompatible,8 has adequate antimicrobial properties,9 excellent flow ability to penetrate within the dentinal tubules10,11 and good adhesiveness.12,13 However, some physical-chemical properties, such as the high solubility and disintegration, and the presence of gaps in the sealer/dentin interface; compromise its performance.12
In many cases, the tooth is not restored in the same session after filling.14 In addition, in several situations, the temporary restorative material used prior to final restoration placement may dislodge from the cavity, compromising the integrity of the root canal recently filled.14 Therefore, it is crucial that root canal sealers are capable to resist to oral fluids leakage for a minimum period, until definitive tooth restoration.14,15
Thus, the aim of this in vitro study was to evaluate the level of coronal microleakage in root canals filled with a MTAbased root canal sealer (MTA Fillapex), in comparison with a calcium hydroxide-based root canal sealer (Sealapex) and an epoxy-amine resin-based root canal sealer (AH Plus). The null hypothesis tested was that there would be no difference among the sealing ability of the sealers, in both periods of analysis.
Materials and methods
For this study, sixty-six freshly extracted human single-rooted teeth, donated by the Bank of Teeth of the Federal University of Amazonas, with prior approval from the Research Ethics Committee (CAAE n.º 36936914.0.0000.5020), were used.
Sample size calculation was performed to determine the number of specimens necessary per experimental and control groups to detect a significant difference of 5% (alpha) among them, for a primary response to a leakage up to 1 mm for control group, and up to 2 mm for the experimental groups; with a mean standard deviation value of 0.5.16
The teeth selected for this study had to be single-rooted, with closed apex, and a 16 mm-long single canal. Teeth that were not in accordance with the selection criteria were eliminated from the final sample.
After samples selection, the teeth were submitted to disinfection process by placing them in 0.5% chloramine T solution at 4°C for 48 hours, followed by washing in running water for 24 hours. Afterwards, the teeth were packed in receptacles containing distilled water at 5°C until use.
Coronal access preparation was performed with spherical- diamond bur No. 1015 (KG Sorensen, Cotia, SP, Brazil) coupled to a high-speed device (MS 400, Dabi Atlante, Ribeirão Preto, SP, Brazil), followed by finishing with cylindrical-diamond bur No. 2135 (KG Sorensen), under constant water cooling.
The root canals were initially negotiated with a size 15 K-type file (Dentsply-Maillefer, Ballaigues, Switzerland), up to the apical foramen, and then, withdrawn to the extent of 1 mm to establish the working length (15 mm). Next, the cervical and middle thirds were enlarged with sizes 2, 3 and 4 Gates-Gliden burs (Dentsply- Maillefer). The apical third was prepared with K3 nickel-titanium rotary system (K3 System, SybronEndo, Orange, CA, USA), in the following sequence of instruments 15.06, 20.06, 25.06, 30.06, 35.06 and 40.06.04/20,.02/20,.04/25,.02/25,.02/30 and.02/35. The root canals were irrigated with 2 mL of 2.5% NaOCl (Rio Química, São José do Rio Preto, SP, Brazil) at each change of instrument.
Afterwards, the smear layer was removed by applying 1 mL of 17% EDTA (Biodinâmica, Ibiporã, PR, Brazil) for 3 minutes, followed by a final irrigation with 2 mL of 2.5% NaOCl (Rio Química).
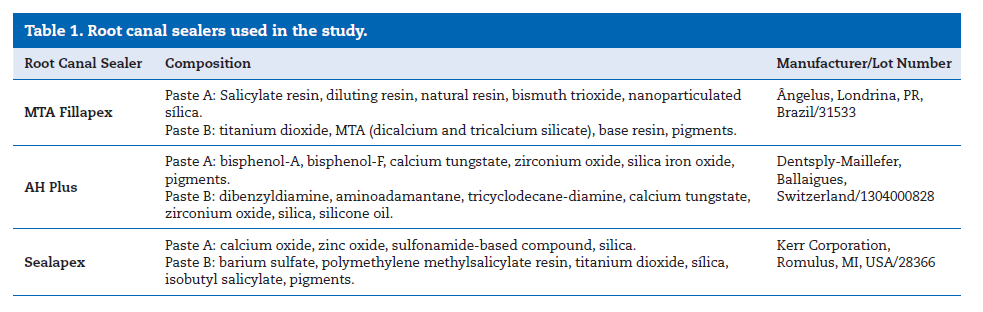
The root canals were aspirated and dried with caliber 40 absorbent paper cones (Dentsply-Maillefer), and then, the teeth were randomly separated into three experimental groups (n=20), according to the sealers used for root canal filling (Table 1):
– Group 1 – AH Plus (Dentsply-Maillefer, Ballaigues, Switzerland).
– Group 2 – MTA Fillapex (Ângelus, Londrina, PR, Brazil).
– Group 3 – Sealapex (Kerr Corporation, Romulus, MI, USA).
The root canals were filled with a size 40 gutta-percha cone (Dentsply-Maillefer) associated to the root canal sealer to be tested, by the Tagger hybrid technique. Thermomechanical compaction of the filling material in the middle and cervical root thirds was performed using a size 60 McSpadden compactor, activated for 10 seconds at 3 mm from the root canal apex. The access cavity of the teeth was not restored to allow sealing ability testing of root canal sealers against the dye solution leakage.
After filling, the teeth were individually packed in receptacles containing artificial saliva, and they were stored in microbiological oven (37°C/100% humidity) for 7 days to simulate the oral conditions. After this period, the root surfaces were coated with 3 layers of cyanoacrylate (SuperBonder Loctite, Aachen, Germany) to prevent dye penetration along the root surface. As the purpose of this study was to evaluate the root canal sealers ability to avoid coronal microleakage, the root canals entrance was not coated. Thus, it was possible to measure the sealing ability of sealers at the coronal level. Six teeth were used as control groups (n =3). Three teeth had their surfaces completely coated with 3 layers of cyanoacrylate, including the root canals entrance (negative control); and three teeth were not coated (positive control).
Next, the teeth were immersed in India ink (Acrilex, São Bernardo do Campo, SP, Brazil) for 15 and 30 days (n = 10). Afterwards, the teeth were washed in running water for 1 hour, dried and cyanoacrylate was removed from the roots surface using a scalpel blade No. 15.
For diaphanization, the teeth were immersed in 5% hydrochloric acid for decalcification. The acid solution was changed every 24 hours until the end of the process. At the end of the decalcification, the teeth were washed in running water for 1 hour to remove any presence of acid solution on the roots surface. Next, the teeth were dehydrated in alcohol (70, 92 and 100%), and then, placed on methyl salicylate to clarification procedure. After diaphanization, the teeth were taken to the operating microscope (40x) (DF Vasconcelos, São Carlos, SP, Brazil) to evaluate the depth of coronal microleakage.
Before microleakage analysis, a single examiner was proper calibrated to prevent misinterpretation of the results. In order to avoid any doubts, coronal microleakage values were measured in millimeters, in a blinded-manner, using as reference the gutta-percha cross section at the root canal entrance, and the longitudinal extent of dye penetration. Thus, the measurements were performed from the root canal entrance to the final point of longitudinal dye penetration. Microleakage measurements were performed three times to ensure the accuracy of the data collected.
The normal distribution of samples was tested (Kolmorov & Smirnov test), and the microleakage values obtained were statistically analyzed (Kruskal-Wallis, p < 0.05) using the Graphpad Prism 4.0 (GraphPad Software, La Jolla, CA, USA).
Results
The graphic representation (mm) for coronal microleakage is in Figures 1 and 2.
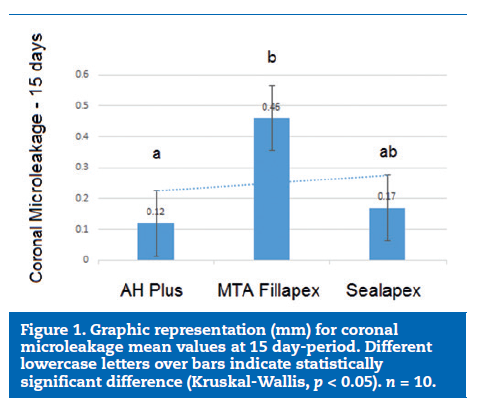
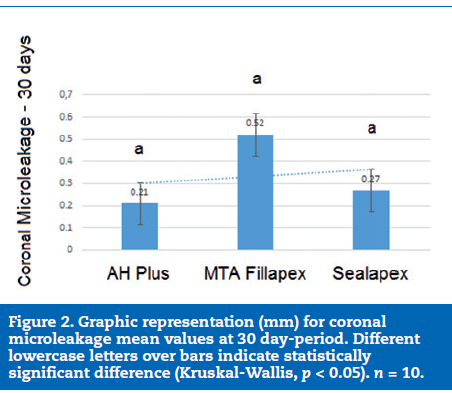
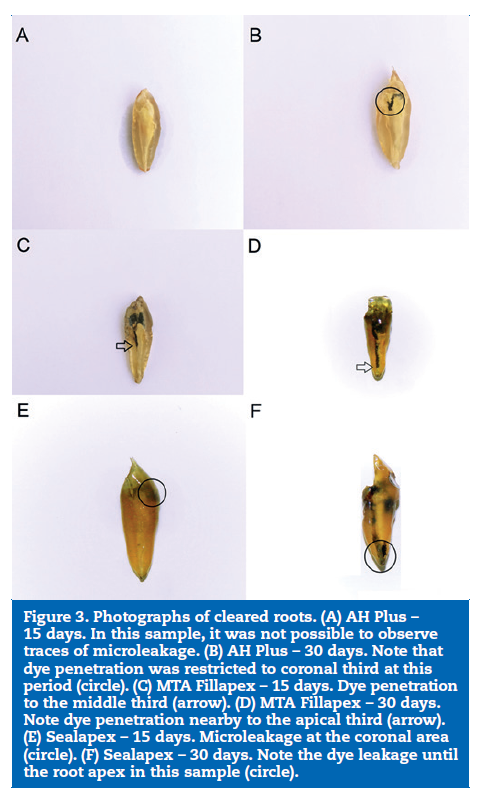
None of the tested root canal sealers was able to prevent coronal microleakage (Figure 3). MTA Fillapex had the highest coronal microleakage values, irrespective of the period of analysis (15 and 30 days). However, these values were significant only in comparison with AH Plus group at 15 days (p < 0.05). In ascending order, the mean values of microleakage at 15-day period of analysis were: AH Plus (0.12 mm), Sealapex (0.17 mm) and MTA Fillapex (0.46 mm). At the 30 day-period, the mean values were 0.21 mm, 0.27 mm and 0.52 mm; respectively.
Discussion
This study evaluated the level of coronal microleakage in root canals filled with MTA Fillapex, in comparison with two root canal sealers of different bases, AH Plus and Sealapex. Based on the results obtained, it can be stated that the null hypotheses was partially accepted, since the tested root canal sealers presented difference in sealing ability only at 15 day-period.
The appearance of several methodologies over the last decades for microleakage analysis, as the use of dye linear leakage and dye extraction, microrganisms penetration, glucose tracer, saliva, radioactive isotopes, fluid transport models and positive pressure systems, were not able to find a valid correlation between in vitro and in vivo studies, impairing the extrapolation of such findings to clinical situations. 17,18 Despite the limitations of microleakage studies, several new materials are launched constantly on the market, making the evaluation of their sealing ability crucial, especially for endodontic sealers.19
The teeth used in the present study were not restored after filling to properly simulate a clinical situation where the restorative material was dislodged from its cavity. Recontamination of root canal system exposed to oral environment demonstrates the importance of an adequate restoration in teeth submitted to endodontic treatment.20 Such exposure of endodontically treated root canals to saliva and microrganisms may lead to necessity of endodontic retreatment.20 For this reason, endodontic sealers must be able to seal the root canal in its entire length, not only apically, but the coronal portion also, preventing microleakage.20
In the present study, MTA Fillapex had the highest mean values of coronal microleakage at 15 and 30 days. Conventional MTA releases calcium ions and phosphorus during its setting process, indicating a possible bioactivity of the cement, as the probable deposition of such compounds on dentin surface increases sealing of the affected area.21 However, MTA Fillapex has a small content of MTA in its composition (13%) (wt), in addition to resinous components, as salicylate, diluents and a natural resin, which compromises calcium ions release.22 This fact might explain the worst performance of MTA Fillapex in comparison with the other root canal sealers tested. Moreover, sealers which contains salicylate in their composition, as MTA Fillapex, may present great contraction during the setting-process, leading to failures in sealer adhesion to root canal walls.23 Significant dimensional changes, such as contraction, may create gaps between dentin and filling material, leading to microbial contamination,23 and a high volume expansion may cause failure in adhesion between root canal sealer and dentin.23 In this case, it is also valid to state that failures in MTA Fillapex/dentin walls interface were observed in 54% of the root canal perimeter in a recent study.11
On the other hand, MTA Fillapex has greater ability to penetrate within the dentinal tubules when cold lateral condensation technique is performed.10 The dentinal tubules penetration of this sealer is proportional to its flow capacity, thereby, determining its effectiveness on filling of root canal in its entire length, including lateral and accessory canals; and possible irregularities in root canal walls.10 In this study, all teeth were filled using a thermoplastic technique, which might have affected the sealer compaction in root canal. Because of the pseudoplastic nature of the sealer, the force used in cold compaction decreases its viscosity, making it to flow more efficiently, and reach critical areas within the root canal.10
Another factor that must be taken into consideration is the solubility of the root canal sealers evaluated. A low solubility facing the organic fluids is essential in order to obtain a durable proper sealing of the root canal system. 14,15 In general, microleakage occurs at the interface between dentinal surface and sealer, sealer and gutta-percha, or sealer itself, because of its dissolution and disintegration with the course of time.14,15
According to the Specification N.º 57 of the American Dental Association (ANSI/ADA),24 the solubility and disintegration of a root canal sealer should not exceed 3% of its initial volume.
Several studies have demonstrated that AH Plus has solubility values lower than recommended by Specification N.º 57,11,25 which might explain the results obtained in this study, as this sealer had the lowest values of coronal microleakage, irrespective of the period of analysis.
On the other hand, recent studies have reported the high dissolution rate of MTA Fillapex.26,27 This root canal sealer presented a solubility higher than 3%, which is not in accordance with the Specification N.º 57 of the ANSI/ADA,24 compromising other physico-chemical properties, as sealing ability. Such higher solubility might lead to sealer particles release, creating gaps and failures in sealer/root canal walls interface, allowing microleakage of fluids and microrganisms within the root canal system.27
Despite the lower levels of coronal microleakage at the 15-day period, the results for Sealapex were statistically similar to MTA Fillapex at both periods of analysis. Calcium hydroxide-based root canal sealers, as Sealapex, are used in endodontic therapy to improve apical repair, as they release calcium ions and promote deposition of mineralized tissue at their site of action.28 Also, studies have reported that Sealapex is able to induce significant apical closure, demonstrating the potential bioactivity of this calcium hydroxide-based sealer,28 which explains its performance as regards to sealing ability.
Few studies have evaluated the sealing ability of MTA Fillapex.
The results obtained so far corroborate the findings of the present study, reporting that this mineral aggregate-based sealer is not able to prevent coronal or apical microleakage.
Conclusions
Microleakage tests have several limitations, such as the effect of root canal anatomy on tests parameters, the difficult in reproducing the in vitro results into
in vivo tests, and the great number of methodologies, which limits the comparison among studies. However, these type of laboratory-based tests are still important to certify new materials, and they have scientific merit under certain circumstances. Despite the limitations of this in vitro study, it can be stated that none of the root canal sealers evaluated was able to prevent coronal microleakage, which increased over the course of time. Furthermore, MTA Fillapex had the worst results at 15 days-period.
References
1. Oliveira SG, Gomes DJ, Costa MH, Sousa ER, Lund RG. Coronal microleakage of endodontically treated teeth with intracanal post exposed to fresh human saliva. J Appl Oral Sci. 2013;21:403-8.
2. Gesi A, Raffaelli O, Goracci C, Pashley DH, Tay FR, Ferrari M. Interfacial strength of resilon and gutta-percha to intraradicular dentin. J Endod. 2005;31:809-13.
3. Panzarini SR, Holland R, Souza V, Poi WR, Sonoda CK, Pedrini D. Mineral trioxide aggregate as a root canal filling material in reimplanted teeth. Microscopic analysis in monkeys. Dent Traumatol. 2007;23:265-72.
4. Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25:197-205.
5. Al-Kahtani A, Shostad S, Schifferle R, Bhambhani S. In vitro evaluation of microleakage of an orthograde apical plug of mineral trioxide aggregate in permanent teeth with simulated immature apices. J Endod. 2005;31:117-9.
6. Vosoughhosseini S, Lotfi M, Shahi S, Baloo H, Mesgariabbasi M, Saghiri MA, Zand V, Rahimi S, Ranjkesh B. Influence of white versus gray mineral trioxide aggregate on inflammatory cells. J Endod. 2008;34:715-7.
7. Prüllage RK, Urban K, Schäfer E, Dammaschke T. Material properties of a tricalcium silicate-containing, a Mineral Trioxide Aggregate-containing, and an epoxy resin-based root canal sealer. J Endod. 2016; 42:1784-8.
8. Assmann E, Böttcher DE, Hoppe CB, Grecca FS, Kopper PM. Evaluation of bone tissue response to a sealer containing mineral trioxide aggregate. J Endod. 2015;41:62-6.
9. Madani ZS, Sefidgar SA, Rashed Mohasel A, Zabihi E, Mesgarani A, Bijani A, Miri SS. Comparative evaluation of antimicrobial activity of two root canal sealers: MTA Fillapex and AH 26. Minerva Stomatol. 2014;63:267-72.
10. Kuçi A, Alaçam T, YavaşO, Ergul-Ulger Z, Kayaoglu G. Sealer penetration into dentinal tubules in the presence or absence of smear layer: a confocal laser scanning microscopic study. J Endod. 2014;40:1627-31.
11. Amoroso-Silva PA, Guimarães BM, Marciano MA, Duarte MA, Cavenago BC, Ordinola-Zapata R, Almeida MM, Moraes IG. Microscopic analysis of the quality of obturation and physical properties of MTA Fillapex. Microsc Res Tech. 2014;77:1031-6.
12. Nagas E, Uyanik MO, Eymirli A, Cehreli ZC, Vallittu PK, Lassila LV, Durmaz V. Dentin moisture conditions affect the adhesion of root canal sealers. J Endod. 2012;38:240-4.
13. Forough Reyhani M, Ghasemi N, Rahimi S, Salem Milani A, Mokhtari H, Shakouie S, Safarvand H. Push-Out Bond Strength of Dorifill, Epiphany and MTA-Fillapex Sealers to Root Canal Dentin with and without Smear Layer. Iran Endod J. 2014;9:246-50.
14. De Castro PH, Pereira JV, Sponchiado EC Jr, Marques AA, Garcia Lda F. Evaluation of marginal leakage of different temporary restorative materials in Endodontics. Contemp Clin Dent. 2013;4:472-5.
15. Schäfer E, Zandbiglari T. Solubility of root-canal sealers in water and artificial saliva. Int Endod J 2003;36:660-669.
16. Julious SA. Sample sizes for clinical trials with normal data. Statist Med. 2004;23:1921-86.
17. De-Deus G. New directions in old leakage methods.... Int Endod J. 2008;41:720-1.
18. De-Deus G. Research that matters – root canal filling and leakage studies. Int Endod J. 2012;45:1063-4.
19. Ahuja L, Jasuja P, Verma KG, Juneja S, Mathur A, Walia R, Kakkar A, Singla M. A comparative evaluation of sealing ability of new MTA based sealers with conventional resin based sealer: an in-vitro study. J Clin Diagn Res. 2016;10:ZC76-9.
20. Oliveira SG, Gomes DJ, Costa MH, Sousa ER, Lund RG. Coronal microleakage of endodontically treated teeth with intracanal post exposed to fresh human saliva. J Appl Oral Sci. 2013;21:403-8.
21. Kim JR, Nosrat A, Fouad AF. Interfacial characteristics of Biodentine and MTA with dentine in simulated body fluid. J Dent. 2015;43:241-7.
22. Viapiana R, Guerreiro-Tanomaru JM, Hungaro-Duarte MA, Tanomaru-Filho M, Camilleri J. Chemical characterization and bioactivity of epoxy resin and Portland cement-based sealers with niobium and zirconium oxide radiopacifiers. Dent Mater. 2014;30:1005-20.
23. Ørstavik D, Nordahl I, Tibballs JE. Dimensional change following setting of root canal sealer materials. Dent Mater 2001;17:512-9.
24. American Dental Association. ANSI/ADA Specification n.º 57 – Endodontic Sealing Material. ADA. 2000.
25. Versiani MA, Carvalho-Junior JR, Padilha MI, Lacey S, Pascon EA, Sousa-Neto MD. A comparative study of physicochemical properties of AH Plus and Epiphany root canal sealants. Int Endod J. 2006;39:464-71.
26. Borges RP, Sousa-Neto MD, Versiani MA, Rached-Júnior FA, De-Deus G, Miranda CE, Pécora JD. Changes in the surface of four calcium silicate-containing endodontic materials and an epoxy resin-based sealer after a solubility test. Int Endod J. 2012;45:419-28.
27. Silva EJ, Accorsi-Mendonça T, Pedrosa AC, Granjeiro JM, Zaia AA. Long-term cytotoxicity, pH and dissolution rate of AH Plus and MTA Fillapex. Braz Dent J. 2016;27:419-23.
28. Holland R, Otoboni Filho JA, Bernabé PF, de Souza V, Nery MJ, Dezan Júnior E. Effect of root canal filling material and level of surgical injury on periodontal healing in dogs. Endod Dent Traumatol. 1998;14:199-205.
Lucas da Fonseca Roberti Garcia
E-mail address: drlucas.garcia@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent.
The authors declare that no patient data appear in this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
Article history:
Received 11 September 2016
Accepted 27 December 2016
Available online 30 March 2017