
Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial
SPEMD | 2019 | 60 (3) | 125-129
Original research
Effectiveness of tongue scraper in reducing halitosis in orthodontic patients: a clinical study
Efetividade do raspador de língua em reduzir a halitose em pacientes ortodônticos: Estudo clínico
a Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, Rio de Janeiro, Brazil
b Pontifícia Universidade Católica do Paraná (PUC-PR), Curitiba, Paraná, Brazil
c Southwest Bahia State University (UESB), Jequié, Bahia, Brazil
Matheus Melo Pithon - matheuspithon@gmail.com
Article Info
Rev Port Estomatol Med Dent Cir Maxilofac
Volume - 60
Issue - 3
Original research
Pages - 125-129
Go to Volume
Article History
Received on 17/04/2019
Accepted on 12/10/2019
Available Online on 29/10/2019
Keywords
Original research
Effectiveness of tongue scraper in reducing halitosis in orthodontic patients: a clinical study
Efetividade do raspador de lingua em reduzir a halitose em pacientes ortodonticos: Estudo clinico
Mônica Gentil Mattosa, Aline de Almeida Nevesa, Orlando Motohiro Tanakab, Lucianne Cople Maiaa, Raildo Silva Coqueiroc, Matheus Melo Pithona,c,*
a Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, Rio de Janeiro, Brazil
b Pontifícia Universidade Católica do Paraná (PUC-PR), Curitiba, Paraná, Brazil
c Southwest Bahia State University (UESB), Jequié, Bahia, Brazil
http://doi.org/10.24873/j.rpemd.2019.10.459
Abstract
Aims:The study aimed to evaluate the effect of tongue-scraping procedures as part of an oral hygiene education program on patients with fixed conventional orthodontic appliances who were affected by oral malodor.
Methods:A sample of 40 fixed-orthodontic patients (14 to 18 years old) was recruited in a private dentistry office. Participants were included in an oral-hygiene education program, and then data were collected, based on interviews, tongue coating detection, and halitosis measurement. After 27 days, these parameters were evaluated again. Data normality was evaluated by the Shapiro-Wilk test for the quantitative variables. The difference between before and after the education intervention was tested by the McNemar test, the Kappa statistic for the categorical variables, and the Wilcoxon test for the quantitative variable. Significance was determined at a 5% (α=0.05) confidence level.
Results:The oral hygiene program applied to orthodontic patients positively impacted on halitosis self-perception, oral malodor measurement (75%), and tongue coating score (100%).
Conclusions:The oral hygiene program, including tongue-scraping procedures, reduced bad odor among orthodontic patients.
Keywords: Halitosis, Oral Health Education, Orthodontics
Resumo
Objetivos:O objetivo do presente estudo foi avaliar o efeito de procedimentos de raspagem de língua como parte de um programa de educação em higiene bucal em pacientes ortodonticos utilizando aparelhos convencionais fixos afetados por mau odor oral.
Métodos:Uma amostra de 40 pacientes ortodonticos fixos (14 a 18 anos) foi recrutada em um consultório odontológico privado. Os participantes foram incluídos em um programa de educação em higiene bucal e, em seguida, os dados foram coletados, com base em entrevistas, deteção de saburra e medicão de halitose. Após 28 dias, esses parâmetros foram avaliados novamente. A normalidade dos dados foi avaliada pelo teste de Shapiro-Wilk para as variáveis quantitativas. A diferença entre antes e depois da intervenção educativa foi testada pelo teste de McNemar, a estatística Kappa para as variáveis categóricas e o teste de Wilcoxon para a variavel quantitativa. A significância foi no nível de confiança de 5% (α=0,05).
Resultados: O programa de higiene bucal aplicado aos pacientes ortodonticos impactou positivamente na autoperceção da halitose, na mensuração do mau hálito (75%) e no escore de saburra (100%).
Conclusões:A utilização de raspador de língua como parte de um programa de educação em higiene bucal reduziu o mal odor entre pacientes ortodonticos.
Palavras-chave: Halitose, Educação em Saúde Bucal, Ortodontia
Introduction
In recent years, improvements in the techniques and materials used in orthodontic therapies have been matched by an increase in undesirable side effects, such as biofilm accumulation, dental enamel demineralization, gingival inflammation, hyperplasia, and also oral malodor.1, 4 Halitosis is the generic term used to describe expired air that has an unpleasant odor, occasionally perceived by the individual themselves, and/or by individuals that socialize with them.5 Its etiology is mostly attributed to an origin in the oral cavity (oral malodor), but it may have other factors, either physiological or psychological, 5 and may even have an extraoral origin.6
Oral malodor results from the proteolytic degradation by microorganisms, which results in the production of organic substrates, including volatile sulfur compounds (VSCs) such as hydrogen sulfite (H2S), methyl mercaptan (CH3SH) and dimethyl sulfide ((CH3)2S).7 Such metabolization occurs predominantly in a coating on the tongue and periodontal pockets.7, 8
The anatomical structure of the tongue, mainly its posterior region, favors the accumulation of debris, thus representing an excellent ecological niche for bacterial proliferation. The presence of a sulcus and papillae generates a microenvironment where the low action of salivary flow and masticatory forces provide reduced levels of oxygen and, thus, anaerobic VSC-producing bacteria have an ecological advantage.9 Taxa isolated from the tongues of individuals with oral malodor include Solobacterium moorei and species that do not proliferate in culture.10
The placement of orthodontic bands and brackets on teeth surfaces favors the deposition of bacterial biofilm, which is the main factor responsible for inflammation in the gingival tissues.11 Although some studies have shown a lower occurrence of oral malodor in patients with self-ligating brackets compared to patients using conventional brackets,12 other studies have indicated that self-ligating brackets have a higher potential for bacterial accumulation.13 Overall, fixed orthodontic therapy interferes with the occurrence of oral malodor due to elevated levels of bleeding, gingival inflammation and the presence of periodontal pockets.13 With this reasoning, studies have focused on exploring the oral malodor etiopathogeny in fixed-orthodontic users, in order to determine their particularities and, consequently, conduct an appropriate control.
Therefore, the present study aimed to evaluate the effect of an oral hygiene program, associated with a tongue-scraping procedure, on patients with conventional fixed orthodontic appliances who had oral malodor. It also aimed to verify the hypothesis that the use of a tongue scraper reduces halitosis in orthodontic patients.
Material and Methods
Before beginning the study, the minimum sample size required for the application of the McNemar and Wilcoxon tests was determined, considering the following parameters: test power of 80% (β=0.20) and error of 5% (α=0.05). For the McNe-mar test, the minimum estimated sample was 38 individuals.
For the Wilcoxon test, initially, a sample calculation for a t-test for paired samples was carried out, and a minimum sample of five individuals was estimated. Subsequently, a 15% increase was applied as an adjustment for the use of non-parametric testing. Thus, the minimum sample size estimated for the application of the Wilcoxon test was six individuals.
The sample calculations were performed using BioEstat (version 5.3, Brazil). A cross-sectional longitudinal study was conducted on 40 orthodontics patients. Before data collection, the project was approved by the Research Ethics Committee of Southwest Bahia State University (number 024-009). The patients and their caregivers gave informed written consent after being explained the study in detail. The participants were 14 to 18 years old and were receiving fixed orthodontic treatment in a private dentistry clinic. Data collection was conducted during regular orthodontic check-ups and included an interview and a clinical evaluation, which were repeated 27 days after the implementation of the oral-health education program.
The inclusion criteria of the study were: (1) dental and skeleton Angle Class I malocclusion; (2) complete permanent dentition; (3) no decay; (4) age between 14 and 18 years old; (5) not presenting anteroinferior crowding higher than 4 mm; and (6) use of conventional fixed orthodontics for 6 to 24 months. The exclusion criteria were the following: 1) presence of gastric disorders; 2) infections in the respiratory tract; 3) anatomical pathologies in the hard or soft oral tissues; 4) any motor deficiency that interfered with performing oral practices; 5) presence of metabolic diseases; 6) presence of systemic diseases; 7) use of medicines; 8) use of mouthwash; and 9) smoking.
The subjects were under fixed orthodontic therapy (Morelli, Sorocaba, Brazil) in both dental arches, with adapted orthodontic rings on the molars, conventional metal brackets bonded to the vestibular teeth surfaces and individual elastic ligatures. The metallic rings were bonded with glass-ionomer dental cement (Vidrion CR, SSWhite, Juiz de Fora, Brazil). All excess cement was removed.
All interviews were conducted by the same clinic, who determined demographic data, frequency of oral hygiene practices, complaints of gingival bleeding, perception of halitosis symptoms when meeting a person for the first time, and self-perception of oral odor, as evaluated on a visual scale from 0 to 100, where 100 represented very good oral odor. A previously calibrated examiner collected all the data. The overall percentage of agreement was 98.16%, and the kappa was 0.89.
For the clinical evaluation of oral odor, the participants were asked not to perform oral hygiene or ingest food, including candy, and drinks two hours before the clinical exam. At baseline, patients were included in an oral-hygiene education program that consisted of professional tooth-brushing (using an Oral BR orthodontic toothbrush), motivation, self-orientation using a fluoride dentifrice, and tongue scraping (CuraproxR CTC203). The same previously trained and calibrated examiner checked for VSCs using a Breath Checker portable device (Tanita Corporation of America, Inc.R, USA), according to the manufacturer’s instructions. Oral odor was classified into five levels: (0) none; (1) slight; (2) moderate; (3) heavy; (4) strong; and (5) intense.
A wooden spatula was used to assess tongue coating. Tongue coating was scored from 0 to 3, as follows: 0 if there was no tongue coating, 1 if it covered less than one-third of the tongue’s dorsum, 2 if it covered one- to two-thirds of the tongue’s dorsum; and 3 if it covered more than twothirds of the tongue’s dorsum. All participants were clinically evaluated at the same time of day, and the rate response was 100%.
Data normality was evaluated using the Shapiro-Wilk test for the quantitative variables. The difference between before and after the education intervention was assessed by the Mc-Nemar test, the kappa statistic for the categorical variables, and the Wilcoxon test for the quantitative variable. Significance was determined at a 5% (α=0.05) confidence level. The data were tabulated and analyzed using the IBM SPSS statistical software version 21.0 for Windows (2012, IBM Corp., Armonk, NY).
Results
The analysis included 40 patients under fixed orthodontic treatment for a period of 6 to 24 months (11.8 ± 3.8 months).
The participants were between 14 and 18 years old (15.5 ± 1.26 years), and 20 were male and 20 female. A total of 38 (95%) of the patients were students, whereas 5% (2) reported other occupations (work or trainee).
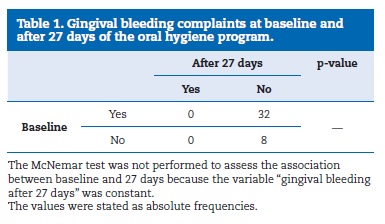
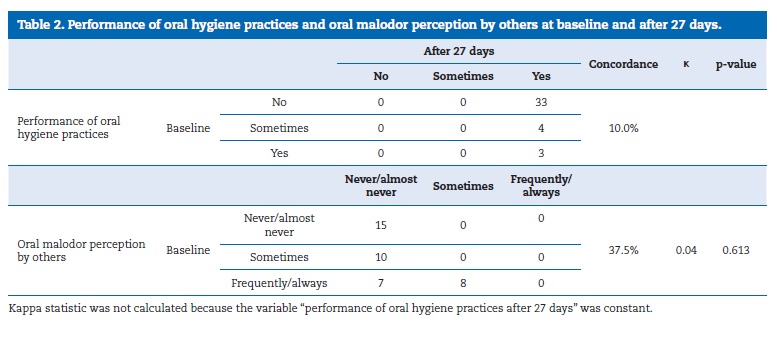
At the baseline, most of the participants (80%) reported gingival bleeding; however, after 27 days of implementation of the oral education program, no participant had that symptom (Table 1). Analysis of the questions concerning oral hygiene practices and oral odor perception by others indicated low adherence between baseline and 27 days after the implementation of the education program (Table 2).
The oral hygiene program impacted the halitosis self-perception, oral odor measurement and tongue coating (Table 3).
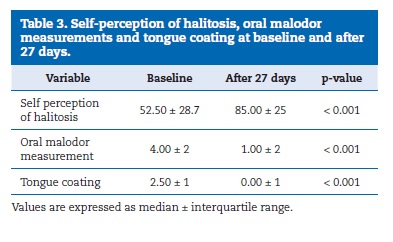
The results highlighted that, after 27 days from the intervention, the fixed-orthodontic patients exhibited a 62% median increase in the self-perceived oral odor score, and a 75% and 100% reduction in oral malodor and tongue-coating scores, respectively.
Discussion
The influence of conventional fixed orthodontic appliances on oral health was investigated based on gingival bleeding, oral health procedures, and oral malodor perception and measurement. Although oral malodor self-perception is a subjective evaluation, the participants followed an objective measuring method.
Gingival bleeding was a prevalent complaint in patients undergoing fixed orthodontic therapy. This finding is mainly attributed to the orthodontic appliance components, which represent an important focus for biofilm accumulation, thereby promoting gingivitis. Despite the taught oral hygiene measures, the clinical study detected moderate gingivitis in all fixed orthodontics patients. In addition, fixed appliances restrict the ability of the tongue and lips to clean the teeth and gingiva mechanically,1, 12 which contributes to a pathological microbial environment associated with a high prevalence of halitosis.
The portable dispositive Breath Checker used in this investigation provided an objective measurement, as well as the advantage of being portable, inexpensive and simple to use.
Recent studies have pointed out that portable devices show good concordance with organoleptic measurements.14 After 27 days, the oral malodor scores had significantly decreased compared to the baseline, although the clinical study indicated an increase after the braces were applied.3, 13 This disparity may be explained by the variability of oral hygiene methodology, considering that the participants were adolescents. Adolescents need a unique approach to be motivated about their oral health issues, which are substantially associated with their social interactions.
Organoleptic measurement has been suggested as the gold standard clinical method for halitosis assessment, but its inherent subjectivity compels the use of other methods.15 Additionally, an interventional clinical study16 has demonstrated that total VSC-level measurement positively correlates with the organoleptic test and tongue-coating scores.
The subjects in this study revealed an excellent improvement following the implementation of the oral education program that was particularly attributed to the routine use of tongue scrapers. The tongue constitutes the largest microcosm of the oral cavity and is inhabited by a highly-diversified body of microorganisms.9 Scientific evidence has demonstrated that mechanical approaches, such as tongue brushing or scraping, have the potential to control oral odor successfully.17, 18 Although studies have pointed out that tongue coating and plaque are increased in fixed-orthodontic patients,19 the present investigation demonstrated a decrease in those indexes 27 days after implementation of the oral education program.
In this investigation, malodor was related to inadequate oral hygiene practices, which is consistent with the findings of other studies; however, those studies did not consider adolescents under orthodontic therapy.20, 21
With regard to the sample’s social demographics, although the subjects had middle education, it was deduced that they were not fully aware of oral malodor etiopathogeny and, consequently, its management.
One limitation of this study was the short time of the follow-up (27 days) since the results could change over a longer period of monitoring. As patients’ oral health practices improve over time, a different oral ecosystem is expected to become established. Orthodontists should be aware that patients under routine therapy may be affected by inappropriate oral health procedures, which can cause oral malodor, leading to personal discomfort and even social embarrassment.20, 22 The hypothesis formulated was confirmed.
Conclusions
Based on the findings of this longitudinal clinical study, the oral hygiene program, including tongue-scraping procedures, is a useful tool for improving oral hygiene in patients with conventional fixed orthodontic appliances who are affected by oral malodor.
References
1. Chang HS, Walsh LJ, Freer TJ. Enamel demineralization during orthodontic treatment. Aetiology and prevention. Aust Dent J. 1997;42:322-7.
2. Nalcaci R, Ozat Y, Cokakoglu S, Turkkahraman H, Onal S, Kaya S. Effect of bracket type on halitosis, periodontal status, and microbial colonization. Angle Orthod. 2014;84:479-85.
3. Babacan H, Sokucu O, Marakoglu I, Ozdemir H, Nalcaci R. Effect of fixed appliances on oral malodor. Am J Orthod Dentofacial Orthop. 2011;139:351-5.
4. Alexander SA. Effects of orthodontic attachments on health of permanent second molars the gingival. Am J Orthod Dentofac Orthop. 1991;100:337-40.
5. Scully C. Halitosis. BMJ Clin Evid. 2014;09:1305.
6. Sanz M, Roldan S, Herrera D. Fundamentals of breath malodour. J Contemp Dent Pract. 2001;2:1-13.
7. Tonzetich J. Direct gas chromatographic analysis of sulphur compounds in mouth air in man. Archs Oral Biol. 1971;16:587-97.
8. Yaegaki K, Sanada K. Volatile sulfur compounds in mouth air from clinically healthy subjects and patients with periodontal disease. J Periodont Res. 1992;27:233-8.
9. Allaker RP, Waite RD, Hickling J, North M, McNab R, Bosma MP, et al. Topographic distribution of bacteria associated with oral malodour on the tongue. Arch Oral Biol. 2008;53(sup.1):S8-S12.
10. Haraszthy VI, Zambon JJ, Sreenivasan PK, Zambon MM, Gerber D, Rego R, et al. Identification of oral bacterial species associated with halitosis. J Am Dent Assoc. 2007;138:1113-20.
11. Ristic M, Vlahovic Svabic M, Sasic M, Zelic O. Effects of fixed orthodontic appliances on subgingival microflora. Int J Dent Hygiene. 2008;6:129-36.
12. Kaygisiz E, Uzuner FD, Yuksel S, Taner L, Culhaoglu R, Sezgin Y, et al. Effects of self-ligating and conventional brackets on halitosis and periodontal conditions. Angle Orthod. 2015;85:468-73.
13. Sokucu O, Akpinar A, Ozdemir H, Birlik M, Calisir M. The effect of fixed appliances on oral malodor from beginning of treatment till 1 year. BMC Oral Health. 2016;16:14.
14. Yilmaz B, Isman O, Aktan AM, Ciftci ME. Evaluation of Halitosis Using Different Malodor Measurement Methods and Subjective Patients’ Opinion Related Own Malodor. Int J Dent Sci Res. 2016;4:72-5.
15. van den Broek AM, Feenstra L, de Baat C. A review of the current literature on aetiology and measurement methods of halitosis. J Dent. 2007;35:627-35.
16. Tanaka M, Anguri H, Nishida N, Ojima M, Nagata H, Shizukuish S. Reliability of clinical parameters for predicting the outcome of oral malodor treatment. J Dent Res. 2003;82:518-22.
17. Van der Sleen MI, Slot DE, Van Trijffel E, Winkel EG, Van der Weijden GA. Effectiveness of mechanical tongue cleaning on breath odour and tongue coating: a systematic review. Int J Dent Hyg. 2010;8:258-68.
18. Casemiro LA, Martins CHG, Carvalho TC, Panzeri H, Lavrador MAS, Pires-de-Souza FCP. Effectiveness of a new toothbrush design versus a conventional tongue scraper in improving breath odor and reducing tongue microbiota. J Appl Oral Sci. 2008;16:271-4.
19. Zurfluh MA, van Waes HJM, Filippi A. The influence of fixed orthodontic appliances on halitosis. Res and Sci. 2013;123:1064-9.
20. AlSadhan SA. Self-perceived halitosis and related factors among adults residing in Riyadh, Saudi Arabia. A cross sectional study. Saudi Dent J. 2016;28:118-23.
21. Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K, Kawaguchi Y. Oral malodor-related parameters in the Chinese general population. J Clin Periodontol. 2006;33 31-6.
22. de Jongh A, van Wijk AJ, Horstman M, de Baat C. Selfperceived halitosis influences social interactions. BMC Oral Health. 2016;16:31.
Matheus Melo Pithon
E-mail address: matheuspithon@gmail.com
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on access to patient data and for its publication.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interest
The authors have no conflicts of interest to declare.
Article history:
Received 17 April 2019
Accepted 12 October 2019
Available online 29 October 2019